|
|
Ainda sobre o swine flu (H1N1) - gripe porcina
|
|
J.TAVARES, MD, FCCP, FAASM
07.12.2009
|
||||||||||
|
||||||||||
Leading the News
CDC review determines H1N1 vaccine to be safe.The New York Times (12/5, A13, Grady) reports that an "extensive review" of the swine flu vaccine has determined that the adverse effects are "no different from those of seasonal flu vaccines." On Friday, CDC director Dr. Thomas R. Frieden called the news "very reassuring," before cautioning that the results "were still preliminary." Dr. Frieden added that the increased potential for developing Guillain-Barre syndrome with this vaccine was "vanishingly remote," although the agency would continue to monitor the adverse effects. Swine flu infections less widespread, vaccine more readily available. The AP (12/4, Stobbe) reported, "Swine flu infections continue to wane, just as vaccine is becoming plentiful enough that some communities are allowing everyone to get it, not just those in priority groups. Swine flu was widespread in only 25 states last week -- mostly in the Northeast and Southwest, officials at the Centers for Disease Control and Prevention said Friday." Seventy-three million doses of vaccine are now available, "roughly twice as much as there was a month ago," and CDC director Dr. Thomas Frieden said that "another 10 million doses are expected in the next week." At least "three states -- Alaska, Arkansas and Oklahoma -- have begun offering swine flu vaccine to all comers." Genetics believed to play a part in swine flu susceptibility. The Minneapolis Star-Tribune (12/6, Marcotty) reported one of the prevailing theories on why the swine flu virus has proved "unexpectedly deadly" for some patients is genetics. Dr. Greg Poland, an infectious-disease expert at the Mayo Clinic, says that some people "inherit an immune system that does not protect them from certain strains of influenza or other infections." Poland says that while many people are not susceptible to the extreme response, "flu viruses are notorious for their ability to mutate," and fears that swine flu "could morph into something lethal to more people." Illinois finds minority populations more at risk for swine flu. The Chicago Tribune (12/5, Mullen) reported, "Blacks and Hispanics in Illinois have died from swine flu at double the rate it has killed whites in the state, and swine flu has hospitalized the two minority populations at more than triple the rate for whites." Illinois officials, citing less access to healthcare and an increased likelihood of chronic health problems as the primary reasons for the discrepancy, "urged minorities to seek out the vaccines." California schools order 23 million masks and gloves for swine flu prevention. The Los Angeles Times (12/5, Hennessy-Fiske, Mehta) reported that millions of masks and gloves intended to help prevent the spread of swine flu "will be distributed throughout California for use by ill students and the nurses who examine them." Meanwhile, Los Angeles County health officials opened the "final dozen H1N1 flu vaccination clinics" in Santa Clarita. County leaders "say they refined their strategy after facing criticism for mismanaging past clinics," and by December 8th, hope to "have distributed nearly 200,000 vaccines at 109 county-sponsored clinics." The AP (12/7) reports that while some counties have reported the pandemic may have peaked locally, California Department of Education spokeswoman Hilary McLean "said schools can always store the masks and gloves in case there's an outbreak of another type of flu."
ResearchLow-calorie diet may reduce obstructive sleep apnea symptoms in obese men.MedPage Today (12/4, Smith) reported that, according to a paper in BMJ, "a low-calorie diet can reduce the symptoms of obstructive sleep apnea in obese patients and in some cases cure the condition." In fact, researchers in Sweden found that "obese men who spent seven weeks on a very low-calorie liquid diet saw their sleep apnea drop from severe or moderate to mild or normal." The paper, accompanying editorialists wrote, "fills a 'major gap' in evidence-based treatment of sleep apnea," considering "only one other randomized trial has looked at the effect of weight loss in sleep apnea." But, "that study did not include men with moderate or severe disease." Regulatory newsFDA warns of Steris sterilizer device malfunction.The AP (12/5) reported, "Doctors and hospitals should stop using a device from Steris Corp. to sterilize surgical tools after reports of malfunction, according to the Food and Drug Administration." The agency said that "users have reported problems" with the Steris System 1 Processor (SS1) sterilizer device "that could result in patients becoming infected from unsterile instruments." The device "has not been cleared as safe and effective." The FDA also received "reports of burns and other injuries sustained by medical staff operating the system," MedPage Today (12/4, Petrochko) reported." Steris made "post-approval changes" to the device, which the FDA said "pose a safety threat to patients and healthcare workers alike." The agency "said it sent the company a warning notification in May 2008, but was not satisfied by the Steris' attempts to switch customers to replacement products." FDA hears proposals on reducing painkiller misusage.In a story appearing in some form on over 360 news websites, the AP (12/4, Perrone) reports that in response to letters issued in February by the Food and Drug Administration requiring risk management plans, "pharmaceutical executives laid out plans Friday to prevent the misuse of prescription painkillers." Industry consultant Sidney Schnoll "warned that mandatory certification standards could cause some physicians to stop prescribing the medications altogether, limiting access to patients." The companies at Friday's meeting suggested that the Drug Enforcement Administration "could offer voluntary training to prescribers." However, FDA leaders, "expressed concern that a key component of the companies' plan relies on congressional action." The Los Angeles Times (12/5, Zajac) "DC Now" blog reported, Dr. John Jenkins, head of the FDA's Office of New Drugs, suggested that the FDA could "institute a voluntary education program for physicians," adding, "I think the challenge for us is there are serious ongoing safety issues with the use of these products that we have to address." Medical device industry said to feel threatened by increased FDA oversight.The Minneapolis Star Tribune (12/7, Moore) reports the med-tech industry is keeping a close eye on the FDA's oversight of medical devices. The Tribune interviews Minneapolis attorney Mark DuVal, who says that the FDA "is getting a lot more risk-averse," and cautions that "it's going to be a lot more expensive and take longer for products to come to the marketplace." He also spotlights the review of the agency's 510k procedure, and says the FDA is "trying to find a solution to something that's not a problem." DuVal warns that altering the program "will drive away venture capital and destroy the robust medical device industry in the United States." General Medical NewsColumnist discusses potential link between certain diseases, endocrine disruptors.Nicholas D. Kristof wrote in a New York Times (12/6, WK11) column that some "public health challenges," like the increased incidence of breast cancer, childhood leukemia, and asthma, may have "to do with contaminants in our water or air -- or in certain plastic containers in our kitchens." Kristof also noted that "it's also well established that Western women are beginning puberty earlier, and going through menopause later." Studies have implicated endocrine disruptors, which "used to be a fringe theory, but it is now being treated with great seriousness by the Endocrine Society." Notably, Rep. "Louise Slaughter...introduced legislation this month that would establish a comprehensive program to monitor endocrine disruptors"
Certain plants appear to remove dangerous airborne contaminants at home.WebMD (12/4, Hendrick) reported that University of Georgia scientists are saying "certain plants can remove dangerous airborne contaminants commonly found in homes" that "have been linked to many illnesses, including asthma, cancer, and reproductive and neurological disorders." According to a paper in HortScience, the "contaminants plants can remove from the air include harmful volatile organic compounds such as benzene, toluene, octane, alpha-pinene, and trichloroethylene." The "five 'super ornamentals' that had the highest rates of contaminant removal" are "the red ivy (Hemigraphis alternata), English ivy (Hedera helix), variegated wax plant (Hoya cornosa), asparagus fern (Asparagus densiflorus), and the purple heart (Tradescantia pallida)." There may, however, "be thousands of [other] plants capable of" phytoremediation. "No one yet knows why some plants are effective at remediation, but...scientists are digging for answers." Law and PolicySenate Democrats target insurance industry pay.The AP (12/5, Werner) reported that Senate Democrats "are taking aim at insurance industry executive pay as they jockey for political advantage in a rare weekend session" on healthcare reform. Republicans, meanwhile, "are showcasing the bill's cuts to Medicare, seeking to undermine support for the legislation among older Americans and others as partisan debate rages over the sweeping remake of one-sixth of the nation's economy." The Washington Post (12/5, Montgomery, Murray) noted that GOP senators "continued their assault" on funding sources for reform, "targeting Democratic plans to cut payments to private insurers who serve Medicare patients and to create a new government insurance program for long-term care that would raise more than $70 billion over the next decade." Democrats" beat back both efforts. They voted 57 to 41 to preserve more than $120 billion in cuts to the Medicare Advantage program." The Senate "also voted to keep provisions to establish the Community Living Assistance Services and Support Act, or Class Act, despite concerns among centrist Democrats that the program would quickly run out of cash." CQ Today (12/7, Vadala, Ethridge) says, "The Senate rejected an amendment to its healthcare overhaul bill Sunday that would limit tax deductions for insurance executives' salaries. In a 56-42 vote, the Senate fell four votes short of the 60-vote threshold needed to adopt the amendment from Blanche Lincoln (D-AR) to limit the amount health insurance companies are allowed to deduct per executive, from $1 million annually to $400,000 annually -- or whatever the compensation of the US President was for that year." Notably, "any savings from the amendment would have been required to go to the Medicare Trust Fund." Medical discrimination laws go into effect.McClatchy (12/7, Hunt) reports the Genetic Information Nondiscrimination Act of 2008 will go into effect on Monday, and will prohibit "insurance companies from using family medical histories or genetic testing to deny medical insurance or set rates." In addition, a separate provision, prohibiting employers from using genetic information in hiring practices, "went into effect Saturday." Linda Robinson, a genetic counselor supervisor with the University of Texas said the new law could "really ease concerns about discrimination that is keeping people from getting these genetic tests."
Michigan Supreme Court to determine role of HIPAA in medical liability case.American Medical News (12/7, Sorrel) reports, "Michigan's Supreme Court is set to decide whether the Health Insurance Portability and Accountability Act preempts a state law allowing defendants in medical liability lawsuits to informally interview plaintiffs' other treating physicians -- a move that doctors say could put them at a disadvantage in defending such cases." In 2008, the Court of Appeals of Michigan ruled that "HIPAA did allow for such meetings, as long as the patient was notified through one of several mechanisms," including a court order. For their part, "physicians say the issue boils down to one of fairness, and rather than using HIPAA to protect patient information, plaintiff lawyers are using it to preclude defendants from obtaining important case details." Plaintiff lawyers, however, "say HIPAA was aimed foremost at protecting patient confidentiality and takes precedence over what they call weaker state laws." Tennessee advocates seek to end exemptions to workplace smoking ban.The Tennessean (12/5, Rau) reported, "Two years after the General Assembly passed a bill to ban smoking from most workplaces, including restaurants, supporters say the law is working and should be extended to include places such as over-21 venues that are now exempt." Advocacy group Campaign for a Healthy and Responsible Tennessee, or CHART, "wants to eliminate exemptions in the law that include allowing smoking at places like 21-and-up establishments, hotel and motel rooms, workplaces with 'garage-door' access, and sites with three or fewer workers." Citing the dangers of second-hand smoke, it is working with state legislators on a bill to be introduced in January to extend the workplace smoking ban, and also hopes to overturn a pre-emption law which bars local governments from adopting their own smoking bans, bar smoking in places where children congregate, and win restoration of $10 million for smoking cessation and prevention programs. Practice ManagementHospital CEOs continue noting physician shortage.American Medical News (12/7, Elliott) reports that according to a recent "report issued by" AMN Healthcare Services Inc., "many clinical professionals, particularly physicians, are in short supply." About "95% of the hospital CEOs" surveyed for the report "said there was a shortage of physicians, with a vacancy rate of 11%, meaning a little more than one in 10 physician job openings are unfilled." Approximately "34% of CEOs had increased the number of physicians on staff within the previous six months, but 46% said patient access to care had been compromised by shortfalls in the number of physicians." Also in the NewsWatson challenges Takeda's Rozerem patent.The AP (12/5) reported that Watson Pharmaceuticals, Inc. announced "it is challenging Takeda Pharmaceutical Co.'s patent on the insomnia treatment Rozerem." Watson is seeking FDA approval for its "8-milligram ramelteon tablets, a generic version of Rozerem, prior to the drug's patent expiration." Takeda has "filed a lawsuit against Watson" seeking to prevent the drugmaker from selling the generic. The suit "will automatically halt "final FDA approval of the generic version for up to 30 months, or until a court makes a final decision." Kaiser to pay $3.75m to settle allegations of false Medicare, Medicaid claims.The AP (12/7) reports, "Four Kaiser healthcare companies have agreed to pay $3.75 million to settle allegations they improperly billed for teaching physicians' services." Federal prosecutors maintain that "from 1996 through 2002 Kaiser falsely billed Medicare" and California's Medicaid program, called Medi-Cal, "for services the companies said had been provided by teaching physicians. The government alleges the services were actually provided by resident physicians without a teaching physician's supervision." The companies involved include "Kaiser Foundation Hospitals, Kaiser Foundation Health Plan, Inc., The Permanente Medical Group and Southern California Permanente Medical Group." The Los Angeles Times (12/4, Girion) noted that payment rules "require providers to record the presence of teaching physicians in patients' records in order to bill for services rendered by residents," and pointed out that this is "not the first time Kaiser has been sanctioned over submitting false bills to the government." HHS report finds rampant Medicare fraud.The AP (12/7, Kennedy) reports, "Miami-Dade County received about half a billion dollars from Medicare in home healthcare payments intended for the sickest patients in 2008, which is more than the rest of the country combined," according to a report from the HHS Office of Inspector General released Monday. Authorities said that in "many cases" Medicare "is billed for services that are never provided." The report also found that Medicare "outlier payments for home healthcare related to diabetes in Miami was eight times the national average." |
||||||||||
Subscriber Tools
Advertise with Custom Briefings:
Reach key professionals every morning
|
||||||||||
|
ATS Morning Minute is a digest of the most important news selected
from thousands of sources by the editors of Custom Briefings. The
American Thoracic Society does not select or edit the news items
contained herein, nor does it receive revenue from any advertising
herein. The views and opinions expressed herein do not necessarily
state or reflect those of the American Thoracic Society, and any
reference to specific commercial products, process, or service by
trade name or otherwise does not constitute or imply an endorsement
by the American Thoracic Society. Neither Custom Briefings nor the
American Thoracic Society is liable for the use of or reliance on
any information contained herein.
This complimentary copy of ATS Morning Minute was sent to jtavares5@aol.com as part of your ATS membership. View Custom Briefings' privacy policy. For more information about other ATS member benefits, please visit www.thoracic.org/sections/membership/member-benefits.html or email membership@thoracic.org. American Thoracic Society | 61 Broadway | New York, NY 10006 Copyright © 2009 by Custom Briefings | 11190 Sunrise Valley Drive, Suite 130 | Reston, VA 20191 |
06.12.2009
"Não percebo porque se deixam as pessoas seduzir por argumentos que não têm profundidade científica. Perante a ameaça de uma disseminação de gripe, a arma mais eficaz que temos à disposição está a ser negligenciada" Dr. Leonardo Ferreira - Pneumologista - In Revista Visão
![]() A
LUTA FINAL CONTRA O H1N1
REVISTA VISÃO Nº 874 de
3 a 9 de Dezembro de 2009
A
LUTA FINAL CONTRA O H1N1
REVISTA VISÃO Nº 874 de
3 a 9 de Dezembro de 2009
Fernando Casimiro (Didinho)
06.12.2009
 Continuando
o debate sobre a gripe H1N1 e bem assim, sobre o sim ou não à vacinação e depois
da análise do Prof. Dr. Joaquim Silva Tavares (Djoca) aos mais recentes
argumentos do Dr. Manuel C. Mendonça (Nhomba), quero dizer que, tal como na
minha anterior intervenção sobre esta matéria, não pretendo fazer finca pé aos
que estudaram medicina.
Continuando
o debate sobre a gripe H1N1 e bem assim, sobre o sim ou não à vacinação e depois
da análise do Prof. Dr. Joaquim Silva Tavares (Djoca) aos mais recentes
argumentos do Dr. Manuel C. Mendonça (Nhomba), quero dizer que, tal como na
minha anterior intervenção sobre esta matéria, não pretendo fazer finca pé aos
que estudaram medicina.
Quando convidei o Prof. Dr. Joaquim Silva Tavares para coordenar o nosso Espaço Saúde, tomei em consideração todo o seu percurso de génio, quer como estudante e professor na Guiné; estudante e médico em Portugal; estudante, investigador e Professor de Medicina, diversas vezes distinguido e premiado nos Estados Unidos da América. Que me desculpem todos os médicos guineenses, independentemente das suas especialidades, qualificações e local onde exercem as suas actividades, mas a Guiné-Bissau, a meu ver, tem na pessoa do Dr. Tavares (como é conhecido nos Estados Unidos), a sua maior referência na área da Medicina!
Considerei também, com relevância, o facto de ser um Homem da Ciência e pela Ciência. A saúde implica responsabilidade e responsabilização, porque é Património Global!
Quero realçar que não estou aqui a tomar partido deste ou daquele, (aliás, quer o Djoca, quer o Nhomba pertencem ao meu núcleo de amigos) mas sim, de teses suficientemente sustentadas com base em argumentos científicos, a Saúde a isso obriga, porquanto ser, no contexto geral, um bem comum, fundamental para a continuidade da nossa existência no planeta Terra!
Na sua primeira abordagem sobre a Gripe A (H1N1), o Dr. Manuel C. Mendonça mostrou-se categoricamente contra a vacinação!
Referindo-se ao início da vacinação na Alemanha, onde reside, disse que" Cerca de 80% da população da Alemanha não quer deixar-se vacinar contra a gripe A, porque não tem nada de anormal.
Disponibilizou uma série de links (nenhum deles de entidades oficiais da área da Saúde na Alemanha, ou da Organização Mundial da Saúde) sobre a questão da Gripe A e da vacinação, para justificar que a Gripe A como doença não é nada de anormal, assim como, para descredibilizar as vacinas produzidas para o combate à Gripe A.
Quanto a mim, O Dr. Manuel C. Mendonça não leu a notícia publicada pela Deutsche Weller no dia 18.10.2009, pois se o tivesse feito, escusaria de dar muitas voltas para (não) encontrar argumentos válidos que justificam a reticência dos alemães para com a vacinação.
É que a Alemanha importou um tipo de vacina para o governo e entidades oficiais, a vacina americana sem aditivos e outro tipo, a vacina europeia, com aditivos, para a população!
É óbvio que esta dualidade de critérios deixou os alemães reticentes, ao ponto de questionarem a vacinação com a vacina produzida na Europa!
Certamente que o mesmo sucederia noutros países, pois não se deve diferenciar as pessoas, para mais, tratando-se de questões de Saúde.
O certo é que pelo Mundo fora, incluindo a Alemanha, os governantes foram vacinados, o que demonstra consideração pela doença e confiança na vacina!
Hoje, e por acompanhar diariamente a evolução da Gripe H1N1 e todas as medidas e recomendações disponibilizadas pelas entidades oficiais de Saúde de todo o Mundo, não posso deixar de dizer que, discordo em absoluto com a forma/conteúdo das intervenções do Dr. Manuel C. Mendonça (Nhomba) neste nosso debate.
Neste nosso site fomentamos o debate de ideias, trocamos opiniões e partilhamos experiências, pois tudo isso é positivo para o exercício mental e para a aprendizagem das pessoas. Porém, não é nossa intenção, nem deve constituir motivação, contrariar a Ciência, seja em que área de actividade for, nem os dados estatísticos ou informativos disponibilizados pelas entidades oficiais, concretamente, na área da Saúde.
Para mim, faltou coerência ao Dr. Nhomba nas suas avaliações, pois, um Doutorado em qualquer especialidade de Medicina, deve ser alguém da Ciência; que acredita nos cientistas, nos estudos científicos, nas entidades oficiais da área da Saúde; que quando não sabe ou tem dúvidas, deve questionar quem sabe, pode e deve dar melhores explicações, e não tentar descredibilizar a Ciência no seu todo e as entidades oficiais de Saúde a nível Mundial, com argumentos infundados e de proveniência não recomendável (os diversos links que acompanharam os seus 2 textos) neste caso, sobre a Gripe A (H1N1).
É caso para perguntar, onde está a deontologia, Dr. Manuel C. Mendonça?!
É que, nas intervenções do Dr. Manuel C. Mendonça, nenhum argumento das entidades oficiais de Saúde, corresponde à verdade, pelo contrário, os links por ele apresentados é que merecem credibilidade sobre a Gripe A (H1N1).
Não cabe em mim o facto de já em Fevereiro deste ano ter recebido uma solicitação de divulgação CURA DO CÂNCER (01.02.2009), por parte do Dr. Manuel C. Mendonça.
Hesitei bastante sobre o assunto e acabei por publicar a referida "notícia" no nosso espaço de divulgação, depois de ter dado a conhecer o seu teor ao Dr. Joaquim Tavares, nosso Coordenador do espaço Saúde, pois oficialmente, nem a Organização Mundial da Saúde (OMS), nem qualquer entidade oficial de Saúde, a nível de países de todo o mundo, reconheceu até hoje, a descoberta da cura do cancro!
Em Agosto passado, o Dr. Manuel C. Mendonça enviou para divulgação o "seu" produto comercial MMS - BALOBA
|
"Caros amigos, conterrâneos e visitantes do www.didinho.org É com imenso prazer que venho através do Contributo divulgar a existência de um site na internet (www.mms-baloba.com), que aborda uma alternativa terapêutica de grande eficácia não só contra o paludismo, como também, contra uma série doutras doenças (febre de Dengue, asma, cancro, artrite reumatóide, tuberculose, hepatite, gripe, herpes Zoster, fibromialgia, etc...). Consulte s.f.f. http://mmsadvisor.com ".
|
Através do CD que o Dr. Manuel C. Mendonça me enviou com o produto MMS - BALOBA, pude ler também que, para além de todas as doenças acima descritas, o milagroso MMS - BALOBA também cura o HIV - SIDA...
|
"Em Uganda registou-se uma efectividade de 60% num grupo de pacientes de HIV, que foram submetidos à um tratamento de 3 dias com o MMS. No espaço de 1 mês, 98% dos doentes estavam já recompostos da doença." |
É ou não um paradoxo, acreditar e querer fazer acreditar a todos que uma solução líquida "milagrosa", denominada MMS - BALOBA, cura uma infinidade de doenças, entre elas algumas que, para a Organização Mundial de Saúde, ainda não têm cura e, inversamente, não acreditar na existência de uma Pandemia, concretamente a Gripe A e nas vacinas disponibilizadas para o seu combate, bem como nos medicamentos de combate quando se contrai a doença?!
Estará o Dr. Manuel C. Mendonça a participar no debate sobre a Gripe H1N1 na qualidade de homem da Ciência, médico (ainda que veterinário), quadro técnico da Indústria Farmacêutica, ou de homem de negócios, com negócio próprio a defender?!
É que gostaria de ter lido algo do Dr. Manuel C. Mendonça no sentido construtivo da busca de soluções para a doença que é uma realidade, que se designou Gripe A (H1N1) e não encontrei nada abonatório nesse sentido...
Gostaria de ter lido aconselhamentos ou sugestões do Dr. Manuel C. Mendonça no sentido de as populações melhor se prevenirem da Gripe A, independentemente da opção que assiste ao doente/utente de aceitar ou não ser vacinado e não encontrei nada sobre o assunto...
Gostaria de ter lido registos oficiais partilhados pelo Dr. Manuel C. Mendonça, sobre a forma como a Gripe A tem evoluído na Alemanha; quais as recomendações e iniciativas das autoridades de Saúde da Alemanha e, acima de tudo, como têm reagido os médicos que lidam diariamente com pessoas contaminadas, mas nada disso encontrei nos escritos do Dr. Manuel C. Mendonça...
Gostaria de ter lido referências a dados oficiais, baseados em estudos e conclusões científicas nos textos do Dr. Manuel C. Mendonça, mas infelizmente, não encontrei nada disso, como se a Saúde que hoje temos no Mundo não fosse definida pelos estudos e aprovações científicas...
Questionar a vacina da Gripe H1N1 como se de um negócio de politiqueiros se tratasse, isto por parte de um Doutorado em Medicina Veterinária, é negar o reconhecimento da evolução de toda a Ciência Médica Mundial.
Quando um Doutorado em Medicina Veterinária diz que a vacina da Gripe não tem o propósito de salvar vidas, esquece-se da acção e dos efeitos de todas as vacinas produzidas até hoje e do empenhamento de todos quanto têm estudado e trabalhado afincadamente para a garantia da existência da raça humana no Mundo!
Falar da Indústria Farmacêutica na primeira pessoa e de forma arrogante, passe a expressão, "E eu acho que quem dispõe das informações de que disponho, nunca há-de estar de acordo com esta nossa vacina.", é de facto lamentável. Quem se julga o Dr. Manuel C. Mendonça, se todo e qualquer medicamento aprovado tem designação, composição e valores aplicados, estando sujeitos a inspecção pelos organismos competentes sempre que necessário?
O que é que o Dr. Manuel C. Mendonça sabe, mas que não dá a conhecer, e que certamente, todos nós gostaríamos de saber?
Espero que este meu ponto de vista sirva para ajudar principalmente os menos informados, no sentido de fazê-los acreditar na Ciência. Nasci numa terra onde ainda hoje a maioria da população não sabe o que é um AVC , quais as suas causas, os sintomas, o que se deve fazer em caso de surgirem os sintomas, etc. , etc.
Uma terra onde a maioria da população continua a desprezar/subestimar, por ignorância, as recomendações das entidades oficiais de Saúde, sendo essa mesma população, a pagar por isso.
Faço questão (pois dei conta de que, por nos ser
acessível neste nosso site, não prestamos o devido reconhecimento ao Professor
Doutor Joaquim Silva Tavares "Djoca") de voltar a partilhar
![]() Dr. Joaquim
Silva Tavares
- Biografia e Currículo
Dr. Joaquim
Silva Tavares
- Biografia e Currículo
Que prossiga o debate!
Vamos continuar a trabalhar!
|
O que urge realçar é a diferença entre a medicina e a indústria farmacêutica. São duas coisas bem distintas. Enquanto a medicina propõe restituir a saúde ao paciente, a farmácia precisa dele doente, para que o negócio nunca mais acabe. Os que conhecem bem este terreno traiçoeiro, resolveram fazer o balanço adequado e deu no que tinha a dar: Uma vaga de protestos contra este tipo de vacina que nos querem impingir, queiramos ou não. E eu acho que quem dispõe das informações de que disponho, nunca há-de estar de acordo com esta nossa vacina.Neste contexto há que ser bem crítico e exigente. Não se deve confiar em tudo que nos contam ou nos mostram. Dr. Manuel C. Mendonça (Nhomba)14 .11.2009
Pandemia ou pandemónio?
Começou hoje a vacinação contra a gripe A na Alemanha e possivelmente também noutros países pelo mundo fora. Cerca de 80% da população da Alemanha não quer deixar-se vacinar contra a gripe A, porque não tem nada de anormal. A Suécia vacinou e de momento a tendência contra a segunda dose é abismal, face às reacções adversas da vacina. A imprensa internacional não fala doutra coisa. Tecnicamente já se está a fugir da denominação gripe suína – um tanto ou quanto sem nexo - porque os suínos, esses sim, ainda continuam sem gripe. O porquê da vacinação já foi sobejamente abordado pelas diversas fontes (independentes) de informação, porque, no que respeita aos doentes que contraíram o vírus, os sintomas em geral são muito leves. Quem estará a tirar proveito deste pandemónio? Porque duma pandemia, cuja definição sofreu uma recente alteração pela parte da OMS a proteger outros interesses, não se pode falar. O que está bem claro neste drama actual, é a necessidade premente de algumas instituições em vacinar o maior número possível de indivíduos. Com que propósito? Salvar vidas? Eis alguns ingredientes da vacina: Mercúrio, Formaldeído, Aspartame, Tiomersal, Fosfato de alumínio, Soro fetal bovino, Transplante de tecido fetal, Células renais do macaco, Glutamato de sódio, etc. Esta mistela nada tem a ver com o propósito de salvar vidas. Que nos contem outras histórias, porque esta já nem um recém-nascido consegue embalar. Não quero aprofundar este tema, mas para facilitar certas informações concretas, deixo aqui ficar alguns Links, cujos conteúdos ainda hão-de fazer arrepiar a pele a um ou outro que ainda acredita, que toda esta encenação tem o mero propósito de nos salvar duma pandemia. Dr. Manuel C. Mendonça (Nhomba)26.10.2009 |
|
Raio de acção do MMS
Este preparado tem um raio de acção quase que ilimitado, quando se considera o seu comportamento oxidante. Para além de oxidar os microrganismos patogénicos ele ainda estimula o sistema imunológico, fortificando-lhe deste modo a auto-defesa natural.
O MMS não é somente eficaz contra uma série de doenças (hepatite, gripe, fibromialgia, herpes Zoster, malária, tuberculose, artrite reumatóide, cancro, tensão arterial alta, sinusite, enxaqueca, dores musculares, etc.. etc..), como também é utilizado e recomendado pela FDA na desinfecção de produtos alimentares (sobretudo carne, frutas e legumes).
O MMS também é utilizado exteriormente para combater doenças da pele originadas por fungos e outros microrganismos. Para curar gengivites e estomatites basta preparar uma solução activada de 6-8 gotas de MMS e com ela lavar a boca e escovar os dentes 4 vezes ao dia durante uma semana.
Conheça e saiba diferenciar os nossos produtos
Devido aos efeitos impressionantes deste preparado no domínio terapêutico, o mercado já começa a ser assediado por produtos falsificados e sem efeito terapêutico. Controle bem a origem do MMS que tiver que comprar. O nosso MMS é produzido na Alemanha, segundo as directrizes recomendadas por Jim Humble, facto este que nos permite usar um certificado do inventor do MMS.
O MMS reage com um activante libertando o dióxido de cloro, conhecido como um dos antimicrobianos de maior eficácia no mundo.
A activação do MMS com um Activante de 50% tem a sua vantagem, porque reduz significativamente o tempo de reacção.
Tanto o nosso MMS (clorito de sódio 28%) como o seu Activante (ácido cítrico 50%) são comercializados em frascos conta-gotas, castanhos, de PET (30 ml, 50 ml e 100 ml), selados e bem vedados.
Deseja encomendar um produto?
Então preencha devidamente o formulário, ou envie um E-Mail para info@mms-baloba.com ou baloba@gmx.net especificando:
♦ o produto e a quantidade que deseja encomendar. ♦ o endereço de entrega da sua encomenda.
Da nossa parte receberá imediatamente por E-Mail uma factura pró-forma, com a totalidade (custo do produto e transporte) a ser transferida para a nossa conta bancária.
Assim que o dinheiro der entrada na nossa conta, enviamos de imediato a sua encomenda para o seu endereço de entrega.
O nosso armazém de Berlim encarrega-se do envio dos produtos via DHL aos nossos clientes. Com a DHL temos uma garantia de entrega imediata ao cliente, assim que o produto chega ao país de destino.
|
20.11.2009
Ainda sobre a controvérsia em relação ao H1N1
Dr. Jorge Herbert
42 anos de idade
Especialista em Medicina Interna
Portugal
“PRIMUM NON NOCERE” – PRIMEIRO NÃO CAUSAR MAL.
 O
título acima não é mais que um aforismo muito aclamado pela classe médica. Há
quem atribui a sua autoria ao pai da Medicina (Hipócrates), mas convém
esclarecer que não consta, pelo menos dito dessa forma, do tão conhecido
Juramento de Hipócrates. Mas existe outra passagem do juramento hipocrático
original que se assemelha a esse aforismo.
O
título acima não é mais que um aforismo muito aclamado pela classe médica. Há
quem atribui a sua autoria ao pai da Medicina (Hipócrates), mas convém
esclarecer que não consta, pelo menos dito dessa forma, do tão conhecido
Juramento de Hipócrates. Mas existe outra passagem do juramento hipocrático
original que se assemelha a esse aforismo.
A medicina baseada na evidência como consequência da evolução tecnológica e do conhecimento médico, o fácil acesso dos doentes às informações disponíveis online e ainda a gestão das instituições hospitalares e clínicas com base em modelos empresariais e todo o interesse económico inerente a essa gestão, vieram claramente alterar a forma como se pratica a medicina, fazendo com que os médicos se distanciem cada vez mais do principal “objecto de trabalho” - o doente ou a população, agarrando-se cada vez mais aos resultados dos exames complementares de diagnóstico e às linhas de orientações baseadas em consensos e estudos, por vezes até a emanações de instituições politicas e politizadas, sem fundamento científico.
Convém referir que a medicina baseada na evidência assenta sobre o pilar de estudos que envolvem um grande número de doentes ou voluntários saudáveis, para se conseguir provar a significância estatística e consequentemente o nível da evidência de cada recomendação. Com isso, quero afirmar que um médico hoje em dia não tem como não se agarrar às evidências para sustentar e alicerçar a sua prática médica quotidiana. Apesar da pressão da indústria farmacêutica em manipular as evidências publicadas, a medicina baseada na evidência é um instrumento útil na orientação do acto médico. É óbvio que em caso de dúvida, o senso clínico deve sobrepor-se sempre às linhas de orientações publicadas.
É importante qualquer médico ter em mente que o princípio de “primum non nocere” deve estar sempre presente em qualquer acto que praticar. Outro princípio básico que deve nortear qualquer clínico é que o doente ou qualquer pessoa que nos procura a solicitar esclarecimentos sobre a sua doença ou um acto médico a que tem de se submeter, deve ser bem informado de todos os riscos e benefícios do referido acto, sem nunca ultrapassar o limite do que o doente/pessoa deseja saber. No momento de informar o doente ou a pessoa interessada, é incorrecto minimizar ou dramatizar o impacto ou a consequência da doença, apenas com o objectivo de manipular a sua decisão.
Como médico, guineense e utilizador do site Contributo, senti-me na obrigação de dar esta pequena contribuição em relação à vacinação para a Gripe A.
Quanto a esse assunto, limito a minha prática diária a respeitar, cumprir e fazer cumprir as orientações técnicas emanadas pelas autoridades do país onde vivo, mas sempre informando os doentes, a luz dos dados disponíveis nos sites médicos de referência e ao encontro daquilo que eles querem saber.
Resumidamente, importa esclarecer as pessoas do seguinte:
Primeiro: o programa da vacinação contra a Gripe A tem como objectivo a prevenção de uma pandemia que poderá acontecer ou não.
Segundo: Enquanto não for declarada estado de pandemia pelas autoridades sanitárias dos países onde vivem, a decisão de tomar ou não a vacina para a gripe A continuará a ser uma decisão individual e deve ser tomada em consciência, depois de devidamente informado e ponderando todos os riscos e benefícios. Ninguém deve ceder a pressões das entidades empregadoras, nem às campanhas de acreditação ou desacreditação da vacina. Até ser oficialmente declarada a pandemia, ninguém deve aceitar assinar qualquer documento a infirmar a aceitação ou negação da vacina, com base na auto-responsabilização por qualquer decisão ou até a inibição da responsabilidade das instituições empregadoras para um eventual contágio no local de trabalho ou por algum efeito secundário grave da referida vacina.
Terceiro: As pessoas devem saber que a gripe A difere da gripe vulgarmente conhecida como “sazonal” essencialmente porque tem mais apetência para o atingimento pulmonar e consequentemente provoca mais síndrome de dificuldade respiratória e risco de internamento numa Unidade de Cuidados Intensivos. Também devem saber que a gripe A não mata mais que a gripe sazonal mas que o seu pico de mortalidade é maior na faixa etária entre os 25 e os 49 anos de idade, essencialmente nas grávidas, pessoas com obesidade mórbida, com doenças crónicas ou algum estado de imunodepressão (vulgarmente conhecida por “defesas baixas”). A gripe sazonal por seu lado mata mais os idosos e principalmente aqueles que têm as mesmas condições de saúde que referi atrás, em relação aos adultos jovens que morrem por gripe A.
Quarto: A população deve saber que não existe nenhum estudo que prova de forma segura a eficácia da vacina contra a gripe A. A eficácia da mesma é inferida em pequenos grupos de pessoas vacinadas e também com base na eficácia dos programas de vacinação de outras vacinas contra outras estirpes do vírus influenza, ou seja da vacina contra a gripe sazonal. Nos EUA espera-se, com o actual programa de vacinação, conseguir vacinar 8.3 milhões de pessoas, para se conseguir obter 75% da eficácia da vacina, prevenir cerca de 1500 mortes e poupar 302 milhões de dólares. Esta quantia será poupada não só na prevenção dos gastos com o tratamento dos casos graves, mas essencialmente com a prevenção do absentismo ao trabalho pelas pessoas infectadas e a consequente redução da produção.
Quinto: É também importante referir aos doentes e à população geral que a grande preocupação com o uso da nova vacina para a eventual pandemia da influenza H1N1 é a segurança, especialmente dado o pouco tempo disponível para realizar ensaios clínicos que permitem provar a tal segurança. Por isso, com excepção de alguns estudos que demonstraram segurança na ausência do atingimento dos fetos na vacinação das grávidas, não existe outro estudo que prova a segurança das vacinas comercializadas para a vacinação contra a gripe A, conforme as normas pré-estabelecidas pelas entidades que aprovam o lançamento dos medicamentos no mercado, dos quais falaremos mais à frente. Em 1976, nos Estados Unidos, cerca de 45 milhões de pessoas foram vacinadas contra o vírus da gripe de origem suína, mas o programa foi prematuramente interrompido, em parte devido a um aumento da incidência do síndrome de Guillain-Barré entre os vacinados.
Não se conseguiu provar a associação directa entre a vacina e o Síndrome de Guillain-Barré, chegando a aventar-se a hipótese dos lotes da vacina usados nesse programa de vacinação estarem contaminados pelo Campylobacter jejunii, que é um agente muito associado a casos do Síndrome de Guillain-Barré. Mas, em 2008, o Sr. Nachamkin e colaboradores, após a análise dos lotes da vacina usada em 1976 e após administrarem vacinas anti-influenza a ratos, publicaram um estudo a negar a contaminação das vacinas utilizadas em 1976 pelo Campylobacter jejuni e ainda afirmaram que a vacina anti-influenza administrada a ratos leva a produção de anticorpos anti-gangliosideos que podem ser responsáveis pela perda da mielina encontrada no Síndrome de Guillain-Barré.
Portanto, tanto a CDC (Centre Disease Control dos EUA), como a FDA (Food and Drugs Administration, também dos EUA), a OMS (Organização Mundial da Saúde) e a EMEA (Agência Europeia do Medicamento) esperam que a vacina contra esta estirpe de Influenza se comporte, em termos de efeitos secundários, da mesma forma que a vacina sazonal, portanto com efeitos secundários ligeiros e em baixo número. Ainda prometem estarem alertas na monitorização de tais efeitos secundários.
Sexto: É relevante esclarecer aos doentes e à população em geral, que a vacina aprovada na Europa não consta da lista das vacinas aprovadas e em uso nos EUA. Há quem afirme (não disponho de dados suficientes para comprovar essa afirmação) que o laboratório que produziu a vacina usada na Europa tentou a aprovação da vacina pelo FDA, mas não conseguiu.
A FDA é a instituição norte-americana que aprova a comercialização dos medicamentos, após a comprovação da sua eficácia e segurança, mandando retirá-los do mercado, se a sua segurança se tornar posteriormente questionável. Na Europa, a instituição responsável por essa aprovação é a EMEA (Agência Europeia do Medicamento). Foi essa instituição que autorizou a comercialização da vacina para a gripe A que está a ser administrada na Europa. No site dessa mesma instituição existe a seguinte afirmação: Pandemrix foi autorizado sob "Circunstâncias Excepcionais". Isto significa que não foi possível obter informação completa sobre a vacina contra a pandemia. A Agência Europeia de Medicamentos irá rever anualmente qualquer nova informação que pode tornar-se disponível e este resumo será actualizado se necessário.
Antes de terminar este meu artigo de opinião, gostaria de reafirmar que a vacinação para a gripe A deve ser uma decisão individual, após correcta informação e ponderação do indivíduo vacinado. Até à fase da declaração do estado de pandemia, em que o interesse da saúde pública sobrepõe-se à integridade individual, o único responsável para a não-vacinação e eventual contracção da doença na sua forma mais grave continua a ser o próprio indivíduo, enquanto a responsabilidade pelos eventuais efeitos secundários graves da vacina, como é óbvio deve ser partilhada pelo próprio indivíduo com a empresa responsável pela produção da vacina, pelas instituições que a aprovaram sem dados que asseguram a sua comercialização em segurança e ainda pelo poder politico de cada país que permitiram a sua utilização massiva.
Também é do meu interesse ser informado sobre as medidas tomadas pela OMS, para acautelar a prevenção da mesma pandemia nos países pobres como é a nossa Guiné-Bissau. Foi criado recursos para a referida prevenção? Temos Serviços de Atendimento a Gripe (SAG) afastado dos outros doentes? As medidas da fase de mitigação estão a ser cumpridas na Guiné-Bissau? Temos um laboratório que faz a confirmação da infecção pelo H1N1? Está a cumprir-se a prescrição do esquema terapêutico e a profilaxia dos conviventes que pertencem ao grupo de risco? Temos stock de Oseltamivir (Tamiflu) que chegue para responder as previsões da infecção pelo vírus H1N1? Existe essa previsão feita pelas autoridades sanitárias guineenses? Faço todas essas perguntas e tremo só de pensar que a resposta pode fazer-me constatar que os nossos irmãos que vivem nesse maravilhoso pedaço de terra não estão incluídos na definição da pandemia, ou seja, que fazem parte de um outro mundo que não o maravilhoso mundo novo de Aldous Huxley.
A todos os meus colegas de profissão, peço desculpa pela superficialidade com que abordei o tema, mas o meu objectivo foi tentar esclarecer os leigos da medicina e disponibilizo-me desde já para qualquer debate aberto e de forma mais aprofundada sobre o assunto. O princípio de “Primum non nocere” e o dever de informar com isenção que tem norteado a minha profissão, não me permitiram manter apenas como espectador.
Fontes:
ü Khazeni, N, Hutton, DW, Garber, AM, Owens, DK. Effectiveness and cost-effectiveness of expanded antiviral prophylaxis and adjuvanted vaccination strategies for an influenza A (H1N1) pandemic. Ann Intern Med 2009
ü Evans, D, Cauchemez, S, Hayden, FG. "Prepandemic" immunization for novel influenza viruses, "swine flu" vaccine, guillain-barre syndrome, and the detection of rare severe adverse events. J Infect Dis 2009; 200:321
ü World Health Organization. Vaccines for the new influenza A(H1N1), 2 May 2009. http://www.who.int/csr/disease/swineflu/frequently_asked_questions/vaccine_preparedness/en/index.html (Accessed May 6, 2009)
ü United States Centers for Disease Control and Prevention. CDC Telebriefing on Investigation of Human Cases of H1N1 Flu, May 28, 2009
ü http://www.cdc.gov/media/transcripts/2009/t090528.htm (Accessed June 2, 2009)
ü Anti-ganglioside antibody induction by swine (A/NJ/1976/H1N1) and other influenza vaccines: insights into vaccine-associated Guillain-Barré syndrome. Nachamkin I, Shadomy SV, Moran AP, Cox N, Fitzgerald C, Ung H, Corcoran AT, Iskander JK, Schonberger LB, Chen RT. J Infect Dis. 2008 Jul 15;198(2):226-33
ü Para quem não for médico e quer saber mais sobre Sindrome de Guillain-Barré, pode consultar a Wikipédia:
http://pt.wikipedia.org/wiki/S%C3%ADndrome_de_Guillain-Barr%C3%A9
14
.11.2009Ainda sobre a controvérsia em relação ao H1N1
 Recebemos
um artigo do nosso irmão Dr. Manuel C. Mendonça (Nhomba) a esclarecer a sua
posição sobre o NÃO à vacinação contra o H1N1. Neste seu artigo, o nosso
ilustre irmão menciona como razão principal do seu posicionamento contra a
vacinação, o uso de aditivos.
Recebemos
um artigo do nosso irmão Dr. Manuel C. Mendonça (Nhomba) a esclarecer a sua
posição sobre o NÃO à vacinação contra o H1N1. Neste seu artigo, o nosso
ilustre irmão menciona como razão principal do seu posicionamento contra a
vacinação, o uso de aditivos.
O uso de 2 aditivos/coadjuvantes na vacina Pandemrix aprovada na Europa.
Os 2 aditivos são o Thimerosal e o Esqualeno.
Por um lado, folguei em saber que ele não é contra a vacinação em geral (pelas nossas correspondências pessoais), mas por outro, ainda estou perturbado pela sua posição contra a vacinação devido ao uso destes aditivos.
Em seguida, vamos falar destes aditivos, com base em artigos do Centro de Controlo de Doenças (CDC), Instituto Nacional de Saúde (NIH) e Direcção para a Administração de Alimento e Medicamentos (FDA - food and drug administration), agências que desde já vos convido a contactar para esclarecimento de qualquer dúvida.
UMA NOTA: “A Vacinação é algo muito sério e o empenho dos cientistas e médicos em promovê-la vem não só da dedicação médica e científica, mas também, da dedicação pessoal, porque a maioria dos médicos/cientistas dedicados ao trabalho com as vacinas também são pais e avós e também põem um tremendo valor na saúde e segurança dos seus descendentes”-CDC
O Thimerosal é um aditivo baseado no mercúrio e que vem sendo utilizado há décadas nos Estados Unidos em algumas embalagens de vacina para doses múltiplas (um frasco pode conter 5 ou mais doses de vacina para o mesmo número de pessoas) para prevenir o crescimento de bactérias e fungos que podem contaminar os frascos.
Desde 2001, nenhuma vacina para crianças com menos de 6 anos, produzida nos Estados Unidos contem Thimerosal: e vacinas de dose única para adultos também nao contêm Thimerosal.
Esqualeno (escassa informação - vinda da OMS)
Aditivo natural, presente em plantas, animais e seres humanos. Pode-se extrair do óleo de pescado. Desde 1977 administraram-se 22 milhões de doses de Esqualeno, sem efeitos nocivos (publicaram-se muitos artigos na Net incluindo os que tentaram relacionar este aditivo com incapacidades em soldados da Guerra do Iraque, vacinados contra o carbúnculo (Essas Vacinas NUNCA CONTIVERAM o Esqualeno!!!)
Para informações sobre a quantidade de Thimerosal (mercúrio) nas vacinas de dose múltipla, podem aceder ao site www.cdc.gov (também mencionamos este tópico no nosso site 2 semanas atrás).
Para os que dizem: Não, não vou introduzir nenhum corpo estranho no meu corpo, lembrem-se que cada dia que voltamos a casa para jantar, o acto de comer e beber neste mundo contaminado é por si só introduzir corpos estranhos no nosso corpo.
A missão de um cientista é questionar, questionar, questionar, e acima de tudo questionar a si mesmo …………….até encontrar a suposta verdade.
Segue o artigo do Dr. Nhomba que tirou parte do seu precioso tempo para pesquisar na Net e encontrar razões para cimentar a sua posição do Não.
Desde já os nossos agradecimentos; Eu particularmente, agradeço-lhe por manter vivo este debate, embora a minha posição do Sim à vacinação será sempre Sim, até me mostrarem evidência Científica plausível, com dados, estudos corroborados por outros estudos independentes, a provar que a vacina é nociva!
Ao chegar a esse ponto, comprarei um bilhete sem regresso ao país dos Medievais e não terei que me preocupar com vacinas, armas nucleares, ventiladores, etc;
Lentamente vou-me deixar consumir pela poliomielite, varíola, varicela, febre-amarela, sarampo, gripe, peste, H1N1,sífilis etc., porque os cientistas são demónios e a Inquisição é quem mais ordena.
Silenciosamente testemunharei a “queimança” na fogueira dos Copernicus, Galileus, Pasteurs, Kochs, Maria Curies, Flemings ……….
Obrigado!
Djoca.
EDITORIAL ESPECIAL DE NOVEMBRO
![]() 06.11.2009
06.11.2009
Manuel C. Mendonça *
14
.11.2009

Caros leitores do www.didinho.org
Como não podia deixar de ser e tendo em conta a actualidade do tema “Gripe Suína”, sinto-me na obrigação de fornecer mais informações, porque este tema é de todos nós, e cada informação, por mais contraditória que seja, pode-nos ajudar a tomar a decisão que acharmos mais acertada.
Antes de tudo agradeço ao Djoca e ao Didinho as opiniões aqui expostas, porque só assim conseguimos formar um juízo sensato, melhorando o nosso trabalho.
O que urge realçar é a diferença entre a medicina e a indústria farmacêutica. São duas coisas bem distintas. Enquanto a medicina propõe restituir a saúde ao paciente, a farmácia precisa dele doente, para que o negócio nunca mais acabe. Os que conhecem bem este terreno traiçoeiro, resolveram fazer o balanço adequado e deu no que tinha a dar:
Uma vaga de protestos contra este tipo de vacina que nos querem impingir, queiramos ou não. E eu acho que quem dispõe das informações
de que disponho, nunca há-de estar de acordo com esta nossa vacina.
Neste contexto há que ser bem crítico e exigente. Não se deve confiar em tudo que nos contam ou nos mostram. Lembro-me duma frase, que, se a memória não me trai, está num aeroporto militar de Israel:
“ Olha bem à tua volta. O avião que não vês, é o que ameaça abater-te”.
Nas minhas deambulações pela NET deparei-me com esta frase do eterno MLK, que muito me sensibilizou:
“Nossas vidas começam a terminar no dia em que nos silenciamos
para as coisas que realmente importam”
M. Luther King
Impulsionado por esta frase , “fiz-me” às fontes e consegui reunir algum material informativo, que só veio a solidificar ainda mais o meu “não” à vacina contra a gripe suína.
O não à vacinação está ligado, por mais contrário que possa parecer, à interpretação científica do produto em causa. Este tema é vasto e acho sensato abordá-lo por partes, para que não seja exaustivo aos leitores menos pacientes.
Assim sendo, quero abordar 3 dos campos interligados neste assunto, que são:
A. O campo “científico”,
B. O campo de “confrontação de interesses” e
C. O campo ligado à “ teoria da conspiração”.
A. O campo científico
O problema principal ligado à rejeição da vacina por médicos, investigadores e outros profissionais da saúde, está ligado directamente à alguns constituintes do produto a ser inoculado.
Em jogo estão principalmente 2 aditivos de “má fama”, conhecidos como
Tiomersal ( também conhecido como Timerosal) e Escualeno.
O Tiomersal é um derivado do mercúrio (49,6%) usado como conservante em certas vacinas (!). È altamente neurotóxico, nefrotóxico, hepatotóxico e cancerígeno. O mercúrio, neste caso o seu derivado, assim que atinge as células cerebrais torna-se irremovível. Tem efeito negativo nas gestantes e influencia o desenvolvimento neurológico dos embriões. Em cada vacina estão 5 microgramas de Tiomersal. Se tiver que receber 2 doses, então ser-lhe-ão inoculados 10 microgramas.
O Tiomersal está sob suspeita de induzir o autismo e a síndrome de Asperger.
Até 1943 o autismo era praticamente desconhecido. Depois com a introdução duma vacina para bébés, com o tiomersal como conservante, explodiram os números de autistas. Com base em resultados de estudos independentes o Tiomersal foi banido da Rússia, do Japão, da Áustria, Dinamarca, Suécia e do Reino Unido. Os outros países ainda continuam a injectar Tiomersal já a começar em bébés de colo (vacinas contra a hepatite B, nalguns casos horas após o parto, e com 2 meses, contra a difteria, têtano e tosse convulsa).
O número de crianças autistas nos EUA explodiu, quando em 1990 foram vacinadas cerca de 40 milhões de crianças com vacinas contendo Tiomersal, que induziu um efeito negativo na fase crítica do desenvolvimento do cérebro das crianças.
Mesmo assim a FDA ainda permite o uso do Tiomersal !!!
O governo americano ainda envia vacinas conservadas com Tiomersal para muitos países em vias de desenvolvimento. A China, que praticamente desconhecia o autismo, tem agora quase 2 milhões de autistas, porque importou em 1999 vacinas americanas contendo Tiomersal.
O Tiomersal foi banido de desinfectantes das mãos já há anos, mas no entanto continua sendo usado nalgumas vacinas (?). Sabe-se lá o porquê de tudo isto?
O Esqualeno reforça a resposta imunológica, reduzindo a quantidade de antígeno viral necessária para a vacinação. Suspeita-se o seu efeito na indução da esclerose lateral amiotrófica. Provoca inflamações crónicas nas articulações (artrite reumatóide), doenças auto-imunes incuráveis de órgãos como o coração, os pulmões, os rins, síndrome da guerra do golfe, dores de cabeça, erupções cutâneas, perda da memória, diarreia, distúrbios neurológicos, etc...
Aqui convém informar que as vacinas empregues nos EUA contra a gripe suína não contêm aditivos. Os americanos devem saber bem o porquê da rejeição dos tais aditivos. Leiam uma das experiências americanas:
Assunto: dados vitais sobre os resultados da U. S. Marinha de vacina contra a gripe suína num navio
Os dados recolhidos indiretamente de depoimentos anónimos de mulheres de Marinha da tripulação afectados através da internet radio show Um fuzileiro naval
Dissertação http://www.clipser.com/watch_video/1362067 :
1. Um navio da Marinha fez-se ao mar em Abril, com uma tripulação de 347 homens
2. Toda a tripulação foi vacinado com a vacina da gripe H1N1.
3. A tripulação adoeceu tão gravemente que outros navios tiveram de responder a prestar auxílio. 16 médicos foram colocados a bordo por um porta-aviões e outros navios anónimos. Um total de 50 funcionários da Marinha foram postos a bordo para responder à crise.
4. Dois dos tripulantes dos 347 morreram - incluindo o capitão do navio (um tenente-comandante) e um suboficial.
5. As 50 pessoas colocadas a bordo para ajudar estão em quarentena no hospital da Marinha em Balboa, Espanha, depois de 10 deles terem contraído gripe da tripulação do navio. Dois dos 50 estão de quarentena em estado grave no último relatório.
6. Da tripulação de 347 que foram vacinados, 333 contraíram a gripe H1N1 da vacina. Dois morreram, como mencionado acima, e 331 sobreviveram. Apenas 14 dos 347 marinheiros vacinados não apresentaram efeitos adversos da vacina.
7. A Marinha ameaçou todos os cônjuges de membros da tripulação do navio de permanecer em silêncio - alegando que toda essa informação está classificada. Alguns são de denúncia e é daí que esta informação é proveniente.
8. No porta-aviões não identificado que prestou assistência, 415 marinheiros contraíram a gripe suína, e estão actualmente de quarentena a bordo.
A verdade é que a epidemia da gripe suína será criada pela vacina.
Se não se deixar vacinar, não haverá epidemia.
A partir deste teste com a tripulação do navio em Abril é evidente que esta vacina é 96% eficaz em infectar o receptor com a gripe suína. Tal taxa de infecção é impossível de alcançar por qualquer meio natural. Embora ela só tenha morto 1% de imediato, não se pode dizer como serão os efeitos da vacina a longo prazo sobre os injetados.
Veja a pesquisa sobre os efeitos a longo prazo da vacina da gripe suína 1976, e a Guerra do Golfo, programas de vacina contra o antraz para mais informações.
De modo que o mero contacto com aqueles que foram vacinados, cria uma probabilidade de 20% de você contrair a gripe suína, mesmo que não tenha sido vacinado.
Falta saber qual foi a vacina empregue neste teste. É fácil supôr que tenha sido uma com um aditivo qualquer. Porque senão, qual haveria de ser a razão da rejeição do Pandemrix nos EUA?
http://forum.pplware.com/showthread.php?tid=3642
Estados Unidos não Aprovam Vacina Gripe A da Europa
EUA recusam vacina para gripe A usada na Europa
A vacina que está a ser usada em Portugal contra a gripe A não foi aprovada
pelos Estados Unidos por conter substâncias na sua composição que podem
alegadamente causar danos à saúde dos que a tomam. Trata-se da Pandemrix, vacina
aprovada pela Organização Mundial da Saúde e escolhida pela Agência Europeia do
Medicamento para ser usada em todos os Estados membros. E em relação à qual o
Infarmed garante terem sido feitos todos os testes de qualidade.
No entanto, a Pandemrix está a provocar a recusa de muitas pessoas na Alemanha
da sua utilização, dando como justificação o facto de os políticos e os
funcionários públicos de topo serem preventivamente vacinados com uma outra. O
presidente do Colégio Alemão dos Médicos de Família refere mesmo que os "potenciais
riscos ultrapassam os benefícios" e, segundo Michael Kochen, este é um "teste em
larga escala feito à população alemã" enquanto o Ministério da Saúde veio a
público esclarecer que a Pandemrix não tem efeitos secundários mais graves que a
vacina alternativa. Segundo o secretário de Estado da Saúde, Klaus Schroeder,
foram encomendadas 50 milhões de doses de Pandemrix e não de outro preparado,
porque pode ser produzida quatro vezes mais rapidamente do que a Cevalpan.
Refira-se que 22 Governos europeus já encomendaram 440 milhões de Pandemrix.
Em Portugal, membros dos grupos prioritários recusaram a vacinação,
designadamente políticos e a classe médica. Ontem, o presidente da Associação
Portuguesa de Bioética, Rui Nunes, considerou que
a recusa de médicos e de outros profissionais
de saúde deve ser aceite com "prudência e bom-senso" porque acha esta
reserva "natural" quando se trata de profissionais que "estão mais envolvidos no
meio; sabem mais do ponto de vista técnico/científico o que se passa e sabem que
não há ainda resultados verdadeiramente sólidos que permitam determinar com
clareza se a pessoa deve ser vacinada".
Nos EUA, a Pandemrix não foi aprovada porque contém uma substância, o
escaleno, que alegadamente provoca a alteração do sistema imunitário. Vários
estudos ligaram os seus efeitos à síndrome da Guerra do Golfo porque terá sido
utilizado como adjuvante na vacina do antrax (ler coluna ao lado). O que está em
causa nesta vacina, segundo os seus detractores, são dois componentes que se
encontram tanto na própria vacina como no adjuvante que lhe é adicionado para
aumentar os efeitos.
Apesar de a vacina da GlaxoSmithKline (GSK) estar em conformidade com as regras
europeias da Organização Mundial de Saúde (OMS), ela contém, segundo a
informação que esteve no site da farmacêutica até ontem a meio do dia, cinco
microgramas de tiomersal - na vacina - e 10, 69 miligramas de escaleno - no
adjuvante -, cujos efeitos secundários são polémicos e considerados
insuficientemente testados nos seres humanos. Estes dois produtos são
necessários para potenciar os efeitos da vacina de modo a que a já gigantesca
produção do medicamento satisfaça a procura em menos tempo de produção. O
escaleno reduz o tempo da cultura de vírus inactivos e o tiomersal permite
utilizar o sistema da multidose.
A preocupação da OMS perante os riscos das vacinas para a H1N1 é tão grande que
responsabiliza as autoridades médicas nacionais para os alegados riscos e
benefícios das vacinas disponíveis antes de as licenciarem, porque "quando
vacinas pandémicas são administradas a tantos milhões de pessoas pode não ser
possível identificar situações raras". Aconselha a monitorização intensa e
comunicação imediata dessas situações e a troca a nível mundial desses dados.
A GSK, contactada pelo DN, considera que no caso do escaleno "não existem
estudos conclusivos que permitam estabelecer relação entre causa e efeito" e
confirma que a substância permite "com menos fazer mais" porque é um
"amplificador de sinal". No caso do tiomersal, refere que "a pequena dose de
mercúrio de 25 microgramas" não "induz malformações no sistema nervoso dos bebés
nem ameaça o de-senvolvimento dos embriões" e que está muito abaixo do "limite
aceitável para as grávidas de 60 kg, que é de 96 microgramas".
O Infarmed - a Autoridade Nacional do Medicamento - confirma que as duas
substâncias encontram-se na Pandemrix, mas que "as afirmações sobre o tiomersal
e o escaleno não são, de facto, nem correctas nem verdadeiras". Esclareceu ao DN
que a vacina foi aprovada por "procedimento centralizado" - pela Agência
Europeia do Medicamento - e que ficou homologada para todos os Estados membros.
O Infarmed informa, também, que "durante o processo de avaliação foram
ponderados todos os aspectos relativos à qualidade, segurança e eficácia de um
medicamento, sendo estabelecida uma relação benefício-risco. Na situação em
apreço, o benefício foi considerado superior ao risco, razão pela qual a Agência
Europeia emitiu uma posição favorável à autorização do medicamento".
In
DN
Para mais informações acerca do campo científico, deixo cá ficar mais alguns Links:
A agência europeia de medicamentos dá a mão à palmatória.
Os profissionais franceses também protestam contra a vacinação em massa.
Aqui convêm conhecer Jane Burgermeister, uma jornalista que se dedica a desmascarar as “outras intenções” da Big Pharmacy.
B. O campo de “confrontação de interesses”
http://www.theoneclickgroup.co.uk/news.php?start=2760&end=2780&view=yes&id=3581#newspost
Patente da vacina da gripe foi registada 1 ano antes da eclosão da epidemia.
http://www.theoneclickgroup.co.uk/documents/vaccines/Baxter%20Vaccine%20Patent%20Application.pdf
Patente da Baxter com requerimento de Agosto de 2008.
http://www.anovaordemmundial.com/2009/10/cientista-da-oms-detem-patente-de-virus.html
Um dos detentores da patente é chefe do laboratório de gripe animal da OMS. Registada 2 meses antes do surto da gripe suína em humanos ?!!
http://www.anovaordemmundial.com/2009/09/epidemiologista-afirma-que-oms-alterou.html
Tom Jefferson, chefe da epidemiologia da International Cochrane Collaboration põe o dedo na ferida e critica a decisão da OMS em mudar a definição da epidemia favorecendo outros interesses.
Normalmente a OMS dá recomendações aos seus membros. Em casos de pandemia, a OMS não dá recomendações, mas sim ordena aos países membros as medidas a tomar.
http://www.youtube.com/watch?v=VWg4GMtqdes&feature=player_embedded
Este vídeo dura 11 minutos, mas vale a pena informar-se acerca das manipulações sem escrúpulos nos bastidores dos todo-poderosos.
Os primeiros casos conhecidos da nova gripe (A/H1N1 estirpe S-OIV)
foram diagnosticados na Califórnia no dia 17.04.2009.
O governo americano declarou no dia 26.04 (9 dias depois) o“estado de emergência sanitária nacional”, quando sómente havia 20 pessoas infectadas com a nova gripe. Também ainda não se tinha registado nem uma morte sequer. No dia 29.04, 12 dias após o diagnóstico dos primeiros casos da nova gripe, a directora-geral da OMS declara a fase 5 da pandemia, ordenando que todos os governos dos estados membros da OMS activassem planos de emergência e de alerta sanitária máxima.
No dia 11 de Junho de 2009 a Dra. Chan declarou a fase 6 da epidemia.
No contexto duma pandemia com a fase 6 é possível:
° Declarar vacina obrigatória, para determinados grupos de pessoas,
inclusivamente para um grupo de cidadãos.
° Decretar a obrigatoriedade. O estado tem a obrigação de fazer
cumprir a lei, impondo multas ou detenções.
Vejam o vídeo em espanhol e formem a vossa opinião acerca da situação actual. Muito informativo.
C. O campo ligado à “teoria da conspiração”
http://www.apfn.org/apfn/aids.pdf
A triste história do HIV. Quero que me digam que é tudo uma brincadeira de mau gosto.
É um documento histórico que merece ser divulgado e bem guardado.
http://www.anovaordemmundial.com/2009/09/len-horowitz-acusacao-formal-ligando.html
Documento muito sério, que, após ter sido confrontado com um mundo de artimanhas, me obrigou a reflectir muito.
Traducao: Blog A Nova Ordem Mundial
LOS ANGELES, CA - Investigadores da indústria farmacêutica
descobriram documentos expondo uma rede de drogas internacional, operando a
partir de Nova Iorque, e que está por trás do pânico da gripe suína e dos
preparativos para a vacinação.
Dr. Leonard G. Horowitz e Sherri Kane, um jornalista de investigação, divulgaram
provas em seus depoimentos a justica que os líderes desta rede global privada de
bio-tecnologia estão por trás da pandemia de gripe, incluindo a sua origem e a
suposta prevenção através de vacinas. Seus documentos, sendo enviados por
advogados para o FBI esta semana, evidencia que estes industrialistas estão
operando uma rede criminosa de dentro da
"Parceria para a cidade de Nova York" (NYCP),
e estão por trás da criação da pandemia, as persuasões da mídia, os preparativos
de vacinação e as promoções de oficiais de saúde .
Dr. Horowitz escreveu aos diretores do FBI: "A rede NYCP, que é de propriedade
de David Rockefeller, envolve vários parceiros poderosos de Wall Street,
incluindo magnatas dos meios de comunicação Ruppert Murdock, Morton Zuckerman,
Thomas Glocer, e o ex-presidente do Conselho de Administração do Federal Reserve
de Nova York, Jerry Speyer, que estão implicados na promoção do genocídio global
".
"Essa "parceria" controla pesquisas em biotecnologia controles de parceria e
desenvolvimento global. Comércio internacional de Saúde também é controlado
quase inteiramente por esta rede, que também exerce o controle quase completo
sobre a mídia de massa para promover/propagandear seus produtos e serviços em
prol do cartel de crime organizado de drogas farmacêuticas. Essa rede, em
essência, é responsável pelo sucesso ou fracasso dos mercados de medicamentos
farmacêuticos e naturais, principalmente através das empresas de mídia de massa
e da propaganda de que dispõe para engenharia social e construção de mercado",
escreveu o Dr. Horowitz.
Entre as revelações da pesquisa de Horowitz e Kane estão as que ligam Larry
Silverstein dona Silverstein Properties, Inc., e os ataques terroristas de 11 de
setembro, as atividades geopolíticas, econômicas e atividades de redução da
população do cartel farmaceutico. Silverstein, proprietário do World Trade
Center, e que autorizou o edifício WTC7 a ser derrubado(detonado) é um dos
principais suspeitos na investigação pelo movimento "9/11 truth". Silverstein é
atualmente co-proprietário e sócio da rede de bio-tecnologia fundada por David
Rockefeller e envolvido nestas novas descobertas.
Dada a natureza sem precedentes e da urgência destes resultados, o Dr. Horowitz
divulgou seu depoimento para a revisão pública no site FLUscam.com, esperando
que a divulgação ampla fará com que os governos mundiais cessem os preparativos
de vacinação em massa para evitar tornar-se cúmplices.
"A última vez que entrei em contato com o FBI eu os adverti sobre os ataques com
antraz iminente uma semana antes das primeiras cartas foram anunciados na
imprensa" (se referindo as cartas com Anthrax logo após aos atentados de 11 de
setembro), o Dr. Horowitz relembra. "Levaram 6 meses para responder. Quando o
fizeram, fizeram-me um suspeito do envio das cartas. Desta vez estou avisando ao
Ministério da Justiça um mês antes do pior genocídio da história. Estou rezando
para que aceitem gentilmente meu apelo para investigarem o NYCP e uma judicial
liminar, para interromper o uso das vacinas para a proteção do público."
O depoimento completo está
neste link
Neste tema da conspiração, aconselho visitar também o site da Jane Burgermeister (www.theflucase.com).
No fim agradeço aos mais pacientes, o tempo dedicado à estas informações, que, a meu ver, hão-de contribuir para elucidar um pouco acerca deste tema muito actual.
Um
grande abraço a todos do vosso NHOMBA
06.11.2009
UMA VISÃO SOCIAL A PROPÓSITO DA GRIPE A (H1N1)
Fernando Casimiro (Didinho)
06.11.2009
Tenho
acompanhado com interesse e preocupação
o evoluir da Gripe A (H1N1), procurando estar diariamente informado sobre a
doença.
Antes de expor o meu ponto de vista sobre o assunto, quero agradecer e felicitar o Djoca e o Nhomba pelas suas distintas contribuições para uma melhor leitura e compreensão da Gripe A (H1N1).
O meu ponto de vista, como anunciado, é uma visão social, contrariamente aos argumentos sustentados por 2 Doutorados em Medicina (ainda que o Nhomba seja Doutorado em Medicina Veterinária), o que quer dizer que não pretendo fazer frente a qualquer dos argumentos partilhados, mas sim, apresentar uma outra visão, que não a de um profissional de saúde, mas de um cidadão, utente dos serviços de saúde.
Sempre ouvi dizer que, com a saúde não se brinca, aliás, tenho algumas e boas razões para concordar com isso. Quando se anuncia uma nova doença, há que ter em conta vários aspectos, fundamentalmente e em primeiro lugar, para não colocar as pessoas em pânico!
Tomando em consideração a questão concreta da Gripe A H1N1 em si e, consequentemente o sim ou não à vacinação, pretendo que este meu ponto de vista sirva para sensibilizar as pessoas no sentido de se valorizar e aceitar a evolução científica do conhecimento humano, como factor de garantia da própria sobrevivência humana num planeta há muito “doente”.
O mundo tem assistido a confrontações de interesses, é certo, mas nunca é demais relembrar Cabral, quando dizia que cada um deve pensar pela sua própria cabeça. Claro está que pensar pela própria cabeça implica formação/conhecimento. Quem se dedica ao exercício do pensamento, da análise, dificilmente se deixa manipular pois tem sempre a possibilidade de fazer diversas leituras e interpretações dos acontecimentos, separando o racional do emotivo.
Quando começaram as mortes no México devido à Gripe A, o mundo assustou-se. Quando a Gripe começou a ser detectada noutras partes do Mundo, concluiu-se que na verdade se estava perante um grande perigo e era necessário contrariar a onda de pânico perante a inexistência de uma vacina testada e aprovada para combater o que já estava a caminhar para a designação de pandemia.
Nessa altura todos desejaram que se "arranjasse" o mais rapidamente uma vacina, pois a Gripe A estava a fazer muitas vítimas e como nestas e noutras situações nenhuma doença selecciona as suas vítimas, houve um grande empenho da Comunidade Médico-Científica Mundial para que se conseguisse uma vacina.
Como não podia deixar de ser, as confrontações de interesses fizeram com que de repente surgissem e fossem sendo partilhadas informações contraditórias sobre a origem da Gripe A, pondo em causa todos os argumentos medico-científicos, não apenas de 1 único país, mas de todo o Mundo, aproveitando a grande ferramenta de Comunicação Global que é a Internet para chegar às pessoas.
Aproveitando-se de certa forma de um certo "controlo" da doença fruto de um trabalho correcto delineado pela Organização Mundial da Saúde, visando conter a propagação da doença, através de campanhas de sensibilização/prevenção e havendo uma ligeira "acalmia" em relação aos receios de uma pandemia, eis que a confrontação de interesses consegue banalizar a Gripe A, ao ponto de manipular os que não pensam por eles próprios, incutindo-lhes a a "teoria da conspiração", como sendo a verdadeira causa do surgimento da Gripe A.
De repente deixou-se de ter receios de morrer de Gripe A e a vacina passou a ser vista como um mal pior do que a própria Gripe.
Não vou escrever muito mais sobre as confrontações de interesses, pois são mais do que evidentes no dia-a-dia relacionado com a Gripe A.
Para mim, o mais importante nisto tudo é que as pessoas devem parar para pensar tendo em conta o seguinte:
A Medicina é uma Ciência dominada por homens e mulheres! São homens e mulheres deste planeta Terra que estudando, cometendo, mas evitando repetir erros, dão garantias de uma vida saudável a todos os habitantes do Planeta. Foram/são homens e mulheres os que derrubaram as maiores barreiras que doenças hoje reduzidas a banalidades colocavam às pessoas. É certo que continuamos ansiosos e esperançados na descoberta, por homens e mulheres deste planeta, de vacinas ou outros medicamentos para a cura de doenças cancerígenas e outras provocadas pelo Sida, Malária etc., etc.
Pergunto: Se há suporte da "teoria da conspiração" na confrontação de interesses, será que alguém ouviu a Comunidade Médico-Científica Mundial anunciar a descoberta de alguma vacina credível, testada e aprovada quer para o cancro, para o Sida e outras doenças até hoje incuráveis?
No entanto, da Comunidade Não Científica já surgiram muitos medicamentos com garantia de cura para todas essas doenças e muitas mais...E o que é que se viu?!
Que milagres realizou a Comunidade Não Científica, quando, mesmo pessoas que se dedicam à Medicina Natural, costumam recorrer aos hospitais?!
Da Comunidade Não Científica que contraria os argumentos da Comunidade Médico-Científica Mundial sobre a Gripe A temos recebido apenas "teses" infundadas, sem qualquer reconhecimento do perigo da doença e, muito menos, respostas concretas e científicas de como prevenir ou tratar algo que existe e mata!
Afinal, qual é o papel, a missão dessa Comunidade Não Científica e como se propõe a ajudar aos que realmente precisam de soluções de prevenção e tratamento da Gripe ou outras doenças?!
É caso para reconhecermos ou não, haver responsabilidade da entidade Mundial da Saúde, a OMS em Geral e dos cientistas de todo o mundo em particular na forma de lidar com as doenças e na busca de soluções para essas mesmas doenças?
Será que havendo a tal "teoria da conspiração", não seria fácil sustentar a origem da Gripe A e outras doenças como sendo actos do terrorismo e daí tirar outros dividendos?!
Será que havendo a tal "teoria da conspiração" países divergentes não teriam há muito denunciado, de forma sustentada, essa "teoria da conspiração"?
Vejamos ainda o seguinte: Num momento em que muitas pessoas em todo o mundo assumem ser contra a vacinação, mesmo sabendo que a vacina só está disponível para grupos prioritários previamente referenciados pela OMS e tomados em linha de conta por cada país, o que aconteceria, ou pode vir a acontecer, caso haja novas mutações do vírus da Gripe A, face à época sazonal de Outono e Inverno por exemplo, numa Europa ponto de encontro e circulação de povos de todos os continentes?!
É que em muitos países as doses de vacinas encomendadas não chegam para o total das suas populações e num caso de emergência, quem acudiria a quem?!
Mais uma questão: Se a Comunidade Médico-Científica Mundial anunciasse um dia destes a descoberta de uma vacina contra o HIV Sida e disponibilizasse essa vacina, argumentando ter sido testada e ser segura, tal como anunciada em relação à vacina para a Gripe A, quantos milhões de seres humanos de todo o mundo, mesmo os menos expostos aos riscos dessa doença não estariam receptivos de imediato a essa vacina?!
É que o mundo aprendeu a respeitar o HIV Sida pelos traços que a doença deixa nas pessoas, o que não acontece no caso da Gripe A, mas não seriam os homens e mulheres, cientistas do nosso planeta a darem esperança de vida e garantias da acção e eficácia dessa vacina?!
Então, por que desvalorizar ou pôr em causa todo o percurso evolutivo do Homem na área mais sensível da existência humana, a Saúde?!
Obviamente que sou a favor da vacinação e como humano tenho orgulho e confiança nos homens e mulheres de todo o mundo que se dedicam às Ciências Médicas!
Vamos continuar a trabalhar!
28.10.2009
Comentários sobre a Gripe Suína (H1N1)
Uma das coisas que mais me
impressionam com o Site Contributo é a oportunidade de debater ideias sobre os
mais diversos assuntos: políticos, científicos, sociais, etc.
Como sabem e como não podia deixar de ser, sou partidário da vacinação contra a gripe (A ou H1N1), e sempre que os doentes ou enfermeiros (as) me pedem conselhos sobre o assunto, recomendo a vacina sem hesitação; Obviamente, a decisão vai pertencer ao paciente e a maioria (mais de 90% seguem o conselho).
Ainda há alguns que, depois de consultarem vários blogues na Internet recusam a vacinação, com o pretexto de tudo ser uma “conspiração” do governo, das companhias farmacêuticas, etc.
Eu, que já vi muitos doentes, jovens, alguns sem condições predisponentes, morrerem nas unidades dos cuidados intensivos por causa desta “doença banal”, ”fantasma”, não vou deixar de apregoar a necessidade da vacinação e das medidas preventivas para evitar a propagação do H1N1 (haverá sempre descrentes: assim aconteceu com a poliomielite e outras doenças que, graças a campanhas de vacinação massiva, foram erradicadas.
Mas temos que dar voz aos que estão do lado oposto, porque não há ninguém que tenha razão a 100%. Há sempre um pouco de verdade ou mentira em qualquer opinião e devemos dar a conhecer aos leitores do Contributo as opiniões dos que estão categoricamente contra a vacina da gripe.
Assim, os próprios leitores poderão formar as suas opiniões e decidirem por si.
Uma palavra: Sempre que leio um artigo “científico”, há inevitavelmente uma lista de questões que coloco:
1-
1- Identificação do autor do artigo: bagagem; artigo independente ou financiado por alguma companhia ou produto.2-
2 - Reprodutibilidade da pesquisa: foi o mesmo trabalho efectuado por indivíduos/instituições distintas, com o mesmo resultado (com alguma margem de erro)?3-
3 - Número de casos maus (se for 0%, temos problemas)4-
4 - Obama factor: 20 dias antes das eleições, consultei alguns blogues nos Estados Unidos: Obama estava 10 pontos atrás de McCain !!!- cuidado com esses blogues. Ainda há blogues, todos os dias com “Obama o anticristo, Obama o Hugo Chavez dos Estados Unidos, Obama comunista, etc.Agradeço ao irmão Nhomba (que está do lado oposto, i.e. o não à vacinação, por ter tido o trabalho de pesquisar na Net e enviar-nos os sites e artigos com comentários pertinentes.
Da minha parte, tomei a minha vacina contra a gripe A 2 meses atrás e a gripe suína (H1N1) hoje.
Junto partilho alguns briefings da American Thoracic Society e artigos selecionados pelo Nhomba e a sua análise pessoal sobre a Gripe Suína.
Obrigado!
Djoca
![]() Prof. Dr. Joaquim
Silva Tavares
Prof. Dr. Joaquim
Silva Tavares
Clique nas imagens para ampliá-las
 |
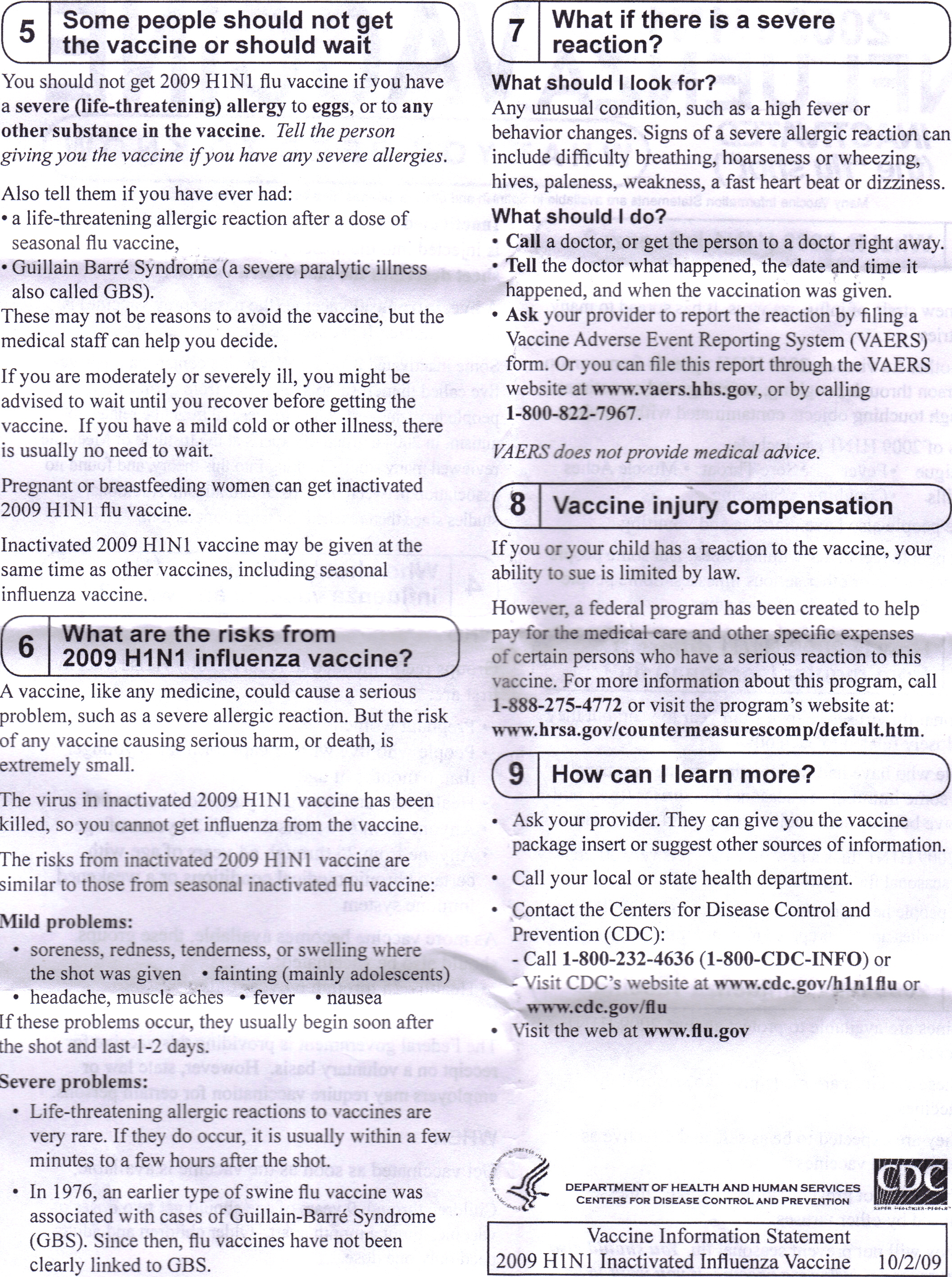 |
|
||||||||
|
||||||||
Leading the News
Sebelius acknowledges vaccine delays.The Washington Post (10/27, Shear, Stein) reports, "Administration officials sought Monday to explain why so much less H1N1 flu vaccine is available than had been promised, blaming the manufacturers and the vagaries of science for nationwide shortages." In interviews Monday, HHS Secretary Kathleen Sebelius said that officials had been "relying on the manufacturers to give us their numbers, and as soon as we got numbers we put them out to the public. It does appear now that those numbers were overly rosy." The New York Times (10/27, A19, McNeil) also notes that Sebelius "promised that, despite delays, there would eventually be enough swine flu vaccine for all Americans." She "appeared on three morning television news programs to deliver the assurance." "Sebelius said she couldn't predict just how widespread the virus will be," the AP (10/27) reports. "But she also said officials do not believe there is yet any cause to close down schools and cease other daily activities." Meanwhile, on CNN Dr. Anne Schuchat, head of the CDC's Immunization and Respiratory Diseases Division, "said it's hard to predict how long the H1N1 wave will continue, so even getting vaccinated a few months from now -- when vaccine supplies are more plentiful -- won't be too late." Reuters (10/27, Zabarenko) says that Sebelius mentioned the possibility of future H1N1 outbreaks, perhaps this spring, saying that a vaccination now would also likely protect against that wave. CBS News (10/27, Morgan) notes that Sebelius "acknowledged the frustration of Americans waiting in lines for vaccinations." She said, "I don't want to minimize the anxiety of a lot of parents who want to get their kids vaccinated, but we do have a vaccine that works." Fauci estimates 150 million vaccine doses delivered by end of year. AFP (10/27) reported that Dr. Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases, said that the US "will face a swine flu vaccine shortfall of 45 to 55 million doses by the end of the year but half of the population could still be vaccinated." He said, "I don't think we will get to the original goal" -- 195 million H1N1 vaccine doses -- but "the government may obtain 140 to 150 million doses, 'which quite frankly I think will likely be enough because we don't anticipate more than half of the people want to get vaccinated.'" More pregnant women getting vaccine. The CBS Evening News (10/26, story 8, 3:00, Smith) reported, "Federal health officials admitted today their projected timetable for producing the vaccine was way off. ... Among those being urged to get the vaccine are pregnant women." CBS correspondent Dr. Jennifer Ashton added, "One hundred pregnant women have been admitted to the ICU across the country with complications of H1N1, 28 have died." She continued, "Traditionally, only about 15% of pregnant women choose to get a regular flu shot and that's because of concerns that they have, understandably so, about putting anything in their body. I am seeing more pregnant patients coming in wanting to be vaccinated against H1N1 and for them...their fear of this virus is greater than any concerns they might have about the vaccine." FDA seeks to curb untested H1N1 remedies. The Washington Post (10/27, Boodman) reports that the Food and Drug Administration has compiled a list of 140 fraudulent swine-flu-fighting products. Gary Coody, the FDA's national health fraud coordinator, says that manufacturers of such products "are motivated by profit, not concern for public health," and said that health officials were concerned that such remedies could delay consumers from seeking genuine medical attention. As a result, "manufacturers are being told to immediately remove unproven claims or unapproved products from their Websites and to respond to warning letters within 48 hours, instead of the usual 15 working days." To date, "more than 90 percent of manufacturers have complied, removing suspect claims, products or, in some cases, entire websites." Schools begin limited vaccination efforts. The New York Times (10/27, A29, Hartocollis) reports, "Despite nationwide shortfalls in the supply of swine flu vaccine, New York City's health commissioner said on Monday that the city was going ahead with the first stage of its plan to vaccinate schoolchildren." According to Dr. Thomas A. Farley, school nurses at 125 small public elementary schools will begin receiving nearly 40,000 doses, which "should be adequate" for now. Dr. Farley added that "as of last week, the city had received about 300,000 of the 380,000 doses of H1N1 vaccine it had ordered, which are being distributed to private physicians, hospitals, public clinics and schools." He also said the city was "optimistic" that the vaccine supply would continue to increase. Hospitals overwhelmed by flu patients may be forced to cancel other services. USA Today (10/27, Sternberg) reports that the "pediatric emergency room at Johns Hopkins Hospital" in Baltimore is seeing "nearly three times as many kids as usual" per day due to the H1N1 flu. But, physicians "at Johns Hopkins and elsewhere expect the number of patients needing hospitalization and intensive care to rise. Such an influx 'could force some hospitals to cancel services such as elective surgery, they say.'" President Obama's national emergency declaration, "designed to give hospitals the flexibility to move patients to satellite facilities" will free up some room, but the unpredictable nature of influenza "makes planning a challenge." Clinical CareCommentary says intermittent smokers should be encouraged to break associations between socializing, tobacco use.The Los Angeles Times (10/26, Stein) "Booster Shots" blog reported, "Smoking-cessation programs typically target frequent smokers with fairly hefty habits," but a commentary published in the Archives of Internal Medicine indicates that "it may be time to also put some focus on occasional and social smokers." Data reveal that "intermittent" smokers "tend to be younger, better educated, better off financially, from minority backgrounds, and are more often female." But, because many of them "consider themselves nonsmokers and, therefore, not at risk for health problems," it's "difficult for healthcare providers to treat them." So, "clinicians must recognize that nondaily smokers, especially social smokers, may be more motivated to quit by messages stressing the harm of secondhand smoke and by encouragement to break associations between social activities and tobacco use rather than by an emphasis on personal health risks." Specific interventions help Pennsylvania physicians curb hospital readmission for patients with chronic lung problems.The Pittsburgh Business Times (10/26, Mamula) reported that, according to 2008 data, "medical care for people with chronic diseases consumes more than 75 cents of every healthcare dollar." In Pennsylvania, "chronic lung problems are the third leading cause of hospital admission." Using Pittsburgh Regional Health Initiative-developed interventions, "dozens of doctors at two large practices have been able to pare hospital readmissions for chronic lung problems within 30 days of discharge by 50 to 75 percent." Besides "hiring nurses to make sure patients understand their medical problems and how to use medications, the PRHI program includes home visits and reminders to make follow-up physician appointments." ResearchRisk for abnormal heart rhythms may be increased following episode of sleep apnea, research suggests.HealthDay (10/26, Edelson) reported that a paper appearing in the Journal of the American College of Cardiology reveals that "the characteristic snorting and gasping of sleep apnea can spur potentially fatal heartbeat abnormalities." After reviewing "nearly 2,900 polysomnograms...of more than 2,500 people," researchers "detected 62 arrhythmias occurring in 57 people with a wide range of sleep apnea disorders." What's more, the "odds of experiencing a heartbeat abnormality were 18 times higher immediately after an episode of sleep apnea than during periods of normal breathing of sleep." The "abnormal heart rhythms," however, "were not linked to the severity of a person's sleep apnea." Regulatory news
GAO report finds drugmakers fail to finish studies on approved drugs.The New York Times (10/27, A18, Harris) reports, "Federal drug officials have long been criticized for failing to force drugmakers to complete studies proving that their drugs work as hoped, and Congressional investigators on Monday released yet another report pointing out that some of these studies remain undone many years after being promised." The Government Accountability Office on Monday released a report which "said that from 1992 through Nov. 20, 2008, the food and drug agency asked drugmakers to complete 144 studies associated with 90 drug applications" under an accelerated-approval program. But "drugmakers had completed just two-thirds of the requested studies." Dr. Joshua Sharfstein, the FDA's principal deputy commissioner, said, "Since getting new powers and funding in 2007, [the] FDA has completely overhauled its system for tracking" these studies, adding, "This is a problem that's being fixed." FDA panel to review CF antibiotic.The San Francisco Business Times (10/26, Leuty) reported, "A Gilead Sciences Inc. investigational antibiotic for cystic fibrosis patients with deadly infections will be reviewed by an FDA panel Dec. 10." The inhalable aztreonam lysine will be reviewed, although "FDA reviewers in September 2008 recommended that the agency not approve the drug, saying that Gilead needed to do more clinical testing. Gilead last week said that a head-to-head study of the drug versus Novartis AG's tobramycin inhalation solution, or TOBI, will be fully enrolled by the end of this year and data from the study will be available in mid-2010." General Medical News
"Family-centered" newborn intensive care units may benefit infants.The Wall Street Journal (10/27, Beck) profiles the newborn intensive-care unit at St. Louis Children's hospital. The unit, called one of the most technologically advanced in the US, is a leader in family-centered care, which welcomes families as part of the medical team. They are allowed in the unit at any time, and their suggestions and observations are encouraged. Small studies have found benefits for the infants under family-centered care, including improved weight gain and less behavioral stress. Law and PolicyReid says Senate bill will include public option with state opt-out.The CBS Evening News (10/26, story 2, 2:15, Cordes) reported, "For months, the public option was declared dead in the Senate," but on Monday, Senate Majority Leader Harry Reid (D-NV) "announced that the contentious government plan would be the cornerstone of the new Senate healthcare reform bill." Sen. Reid said, "The public option can achieve the goal of bringing meaningful reform to our broken system." NBC Nightly News (10/26, story 5, 1:15, O'Donnell) reported, "Leaders of both parties had predicted that a public option was dead. But tonight it is back, and Senate Majority Leader Harry Reid is taking a risk." But "for more liberal Democrats, this kind of public option or any kind of public option is considered a victory." On ABC World News (10/26, story 5, 2:45, Gibson), George Stephanopoulos said Reid "still may not have the votes to get this to the Senate floor. But what the Senate leader saw is that he would have a lot more trouble with the majority of Democrats if he didn't include the public option in the bill than if he did." USA Today (10/27, Fritze) reports the "latest iteration of the public option would give millions of Americans who are not covered through their employer the option to buy insurance run by the government. States would have until 2014 to decide whether to withdraw from the public program, which Reid says would drive down rates." According to Bloomberg News (10/27, Litvan, Rowley), Reid "said the so-called public option with the opt-out provision is the 'fairest way to go' to ensure competition for private insurers." The New York Times (10/27, A1, Pear, Herszenhorn) reports in a front-page story that Reid "sided with his party's liberals," but the announcement "set the stage for a test of Democratic party unity. With Republicans united for now in opposition to any bill including a public option, Mr. Reid needs support from all members of his caucus -- 58 Democrats and two independents -- to take up the legislation." AFP (10/27, Knox) says that Reid "said the public option was 'not a silver bullet' but pointed to recent public opinion polls that showed a majority of Americans support the option to pick a government-backed insurance plan." The Washington Post (10/27, Murray, Montgomery), the Los Angeles Times (10/27, Levey), the Washington Times (10/27, Haberkorn), The Hill (10/27, Young), the Wall Street Journal (10/27, A1, Hitt, Adamy), and Roll Call (10/27, Drucker) also cover the story. Clove cigarette ban seen as being in legal limbo.In a front-page story, the Wall Street Journal (10/27, A1, Newman) reports on kreteks, or clove cigarettes, which were recently banned by the FDA. After the ban, many kretek manufacturers soon released clove cigars, a similar product. After the FDA announced that kreteks could also fall under the ban if they fit the profile of a cigarette, a California kretek importer sued the agency, accusing the FDA of "deliberately obfuscating" the "definition of cigarette." Should that effort fail, the Journal notes that Indonesia could file a complaint with the World Trade Organization, on account that the US law bans cloves but allows menthol cigarettes. Practice Management
Physicians should invest time in research before prescribing off-label, experts say.The Los Angeles Times (10/26, Healy) "Booster Shots" blog reported that prescribing "drugs...for a use other than that approved by the" FDA is "perfectly legal, though patients are largely in the dark about what 'indications' or uses the FDA has approved for different prescription medications." Federal law prohibits drugmakers from promoting drugs "for 'off-label' purposes," but "the practice means big money for" them, "and some do it anyway." But, "these 'off-label uses' have not been scrutinized...for safety and effectiveness." In a commentary in the Archives of Internal Medicine, "three writers from the National Institutes of Health" urged physicians to "do a little research before writing off-label; think twice before offering something that's new to the market, carries risks of dangerous side effects, or is very expensive; in most cases, acknowledge uncertainties to the patient; and share what you've learned with other doctors." Also in the NewsRequired hospital reporting seen as viable way to reduce preventable infections, events.The Wall Street Journal (10/27, Goldstein) notes that a study published three years ago showed how more than 100 ICUs in Michigan hospitals significantly lowered their rates of hospital-acquired bloodstream infections by following a simple five-step checklist, but information on hospitals using the checklist has been limited. In an interview with the Journal, the study's leader, Peter Pronovost, now at Johns Hopkins, said that a survey requested earlier this year by Rep. Henry A. Waxman (D-CA) showed that all 50 states were using the checklist, but only 11 were actually measuring infection rates. Pronovost believes the checklist will only provide meaningful results if hospitals are required to report their infection rates. In a separate article, the Wall Street Journal (10/27, Simon) provides a 10-step list to prevent infections in healthcare settings, which it says it compiled by talking with providers, and with information from the Committee to Reduce Infection Deaths and the Association for Professionals in Infection Control and Epidemiology. The list includes such things as using undercover agents and computer surveillance to requiring workers to use chlorhexidine glutonate soap. The Journal also recommends requiring hospitals to report their rates, and points out that only 25 states have such laws. |
||||||||
Subscriber Tools
Advertise with Custom Briefings:
Reach key professionals every morning
|
||||||||
|
ATS Morning Minute is a digest of the most important news selected
from thousands of sources by the editors of Custom Briefings. The
American Thoracic Society does not select or edit the news items
contained herein, nor does it receive revenue from any advertising
herein. The views and opinions expressed herein do not necessarily
state or reflect those of the American Thoracic Society, and any
reference to specific commercial products, process, or service by
trade name or otherwise does not constitute or imply an endorsement
by the American Thoracic Society. Neither Custom Briefings nor the
American Thoracic Society is liable for the use of or reliance on
any information contained herein.
This complimentary copy of ATS Morning Minute was sent to jtavares5@aol.com as part of your ATS membership. View Custom Briefings' privacy policy. For more information about other ATS member benefits, please visit www.thoracic.org/sections/membership/benefits-of-an-ats-member.html or email membership@thoracic.org. American Thoracic Society | 61 Broadway | New York, NY 10006 Copyright © 2009 by Custom Briefings | 11190 Sunrise Valley Drive, Suite 130 | Reston, VA 20191 |
|
||||||
|
||||||
Leading the News
Obama declares H1N1 outbreak a national emergency.The AP (10/25, Elliott) reported that President Obama "declared the swine flu outbreak a national emergency, giving his health chief the power to let hospitals move emergency rooms offsite to speed treatment and protect noninfected patients." The declaration, signed Friday night and announced Saturday, "comes with the disease more prevalent than ever in the country and production delays undercutting the government's initial, optimistic estimates that as many as 120 million doses of the vaccine could be available by mid-October." The Los Angeles Times (10/25, Hook) reported that the declaration gives Health and Human Services Secretary Kathleen Sebelius "temporary authority to grant waivers that would expedite steps such as setting up off-site emergency rooms to treat potential flu victims apart from other patients." In a front-page story, the Washington Post (10/25, A1, Shear, Stein) reported White House spokesman Reid Cherlin said the waivers "may be granted only to healthcare facilities that request them. 'Adding a potential delay while waiting for a National Emergency Declaration is not in the best interest of the public, particularly if this step can be done proactively as we are doing here,' he said." Bloomberg News (10/25, Pollack, Brower) reported the flu "is now widespread in 46 states and accounts for 411 confirmed deaths since Aug. 30 and more than 8,200 hospitalizations, according to the Centers for Disease Control and Prevention. The numbers reflect what would be the peak of a typical flu season, CDC Director Thomas Frieden, said Oct. 23. 'Many millions of cases' have occurred in the US since the outbreak began earlier this year, he said." Emergency decree comes as vaccine delays continue. The CBS Evening News (10/25, story 3, 2:20, Mitchell) reported, "Health officials batting the H1N1 flu virus this weekend have received two booster shots of their own. President Obama has declared the virus a national emergency, a move that cuts bureaucratic red tape. And, the FDA has approved emergency use of the experimental anti-viral drug Peramivir. With the outbreak now touching 46 states, the new help comes not a moment too soon." ABC World News (10/25, story 6, 2:05, Harris) reported that an "unintended consequence" of Obama's declaration of national emergency is that "some people are panicking." ABC added, "Doctors tell us that about 100 people under the age of 18 have died so far this year of swine flu. That's compared to about half as many in any other average flu year." NBC Nightly News (10/25, lead story, 2:30, Holt) reported, "The government says that declaration does not signal cause for greater alarm, but simply gives it a freer hand to respond to the crisis. Surprisingly, however, calling it an emergency does not solve the most pressing concern, a big shortfall in the amount of flu vaccine available." Of the emergency declaration, HHS' Nicole Lurie said, "More people are getting sick, more people are going to the hospital, more people are dying and we wanted to be prepared in case hospitals got a lot busier or more overwhelmed." Still, NBC (Yang) added, "The national emergency declaration does nothing for vaccine production." Dr. Lurie said, "Hang on, be patient, vaccine is coming." The Wall Street Journal (10/26, A3, McKay, et al.) reports that Novartis blamed some of the vaccine delays on HHS for changing its vaccine order, and requesting "more single-dose syringes" due to thimerosal fears. Bruce Gellin, director of the National Vaccine Program Office, said, however, "HHS has never issued or discussed a new delivery order or a modification to an existing delivery order that would increase the number of pre-filled syringes and delay supplies to the US public." The New York Times (10/26, Calmes, McNeil) also covers the story. Over 1,000 Americans have now died of H1N1 flu. ABC World News (10/23, story 4, Gibson) reported, "The government said today that H1N1 flu has caused more than 1,000 deaths, and its spread matches the illness rate normally seen at the peak of the regular flu season." The CBS Evening News (10/23, story 2, Couric) reported the flu is "widespread now in all but four states. Since April, at least 95 children have died. To put that number in perspective, that's just over one in a million American kids." NBC Nightly News (10/23, story 2, Williams) reported that the flu is "galloping its way across the country, hitting mostly young people, including 95 percent of the college campuses in this country. Those waiting for the vaccine got some bad news from the federal government today, but a lucky few also got what they came for." The Wall Street Journal (10/24, A1, McKay, Dooren) reported on the shortage in supply of the vaccine. The AP (10/23, Stobbe) reported, "More Americans have been vaccinated against seasonal flu this fall than ever before by this time of year, federal health officials said Friday. Sixty million people have gotten the winter flu vaccine -- probably because they're paying more attention to flu warnings in general, thanks to swine flu. It's an unprecedented number of seasonal flu shots for October; most usually aren't given until later in the fall." FDA approves anti-viral for emergency use. The CBS Evening News (10/25, story 3, 2:20, Mitchell) reported, "The FDA has approved emergency use of the experimental anti-viral drug Peramivir." CBS (Pinkston) added that the drug "has already been given to at least eight people who were near death from H1N1. They survived." The Wall Street Journal (10/26, Dooren) reports that the FDA is allowing Peramivir to be used to create H1N1 vaccines. However, the agency says that only limited clinical data on the drug's safety and effectiveness are available, although it approved the emergency use that the request of the CDC. NYTimes calls suspension of health worker vaccination rule "a mistake." The New York Times (10/24, A20) editorialized, "Gov. David Paterson of New York and his health commissioner have suspended a pioneering regulation that required all healthcare workers to get vaccinated for the flu -- both the seasonal flu and the new swine flu. It is a mistake, and New Yorkers, especially those in hospitals, could pay a high price for it. The Paterson administration says it needed to save scarce vaccine supplies for the most vulnerable people," but others "suspect the administration had given in to the fierce objections of healthcare workers and their unions." Clinical CarePatients may have trouble controlling asthma due to lack of medication adherence, investigators say.The Los Angeles Times (10/24, Stein) "Booster Shots" blog reported, "Asthma can be a tough condition to treat in certain patients," but a paper appearing in the American Journal of Respiratory and Critical Care Medicine suggests that the "difficulty may sometimes lie with the patients, not the medication." After analyzing data on 182 patients, which included "refill rates" over the course of six months, investigators noted that "people don't always adhere to the prescribed dosages for inhaled and oral asthma medication, even when they say they do." In fact, "among patients prescribed a maintenance course of oral steroid, the blood analysis showed that nearly half (45 percent) were not taking their medication as prescribed," WebMD (10/23, Boyles) reported. "And, more than half of these patients (65 percent) were also noncompliant with their inhaled treatment," with women being more likely to stray from their regimen. Notably, "all of the poorly compliant patients had initially denied taking less of their medications than they were prescribed." Research
Research suggests women may be more vulnerable to cigarette carcinogens.HealthDay (10/25, Doheny) reported, "Women may be more vulnerable than men to the carcinogens and other noxious substances in cigarette smoke, a growing body of research suggests." For instance, through their study of some 700 people, Swiss scientists noted that "women tended to be younger when they received the diagnosis, even though they smoked less than the men who developed lung cancer." Although "actual evidence suggests that men and women are remarkably similar in their" lung cancer risk, an American Cancer Society expert pointed out that the "types of lung cancer they get are different." Meanwhile, a team comprised of Harvard and Norwegian researchers discovered that "women with COPD were younger when they got the diagnosis and had smoked less than the men with the respiratory ailment." P/F ratio may indicate potential VILI in patients undergoing general anesthesia, study indicates.Medscape (10/23, Helwick) reported, "In patients without existing lung injury, ventilator-induced lung injury (VILI) occurs in 24 percent after five days of ventilation. The ratio of arterial oxygen concentration to the fraction of inspired oxygen (P/F ratio) is one of three criteria for lung injury." University of Michigan researchers concluded that "might be a marker of potential VILI in patients undergoing general anesthesia" after conducting a "retrospective study of all adults undergoing general anesthesia over a three-year period, excluding cardiac and thoracic procedures and patients classified as ASA 4 or 5 (i.e., with serious/life threatening systemic disease)." Patients with a "P/F ratio of less than 300 at baseline were excluded, and those with a subsequent P/F ratio of less than 300 during anesthesia were identified as having potential VILI." Regulatory newsGAO says FDA fails to follow up on unproven drugs on the market.The AP (10/26, Perrone) reports that a GAO report due Monday says the FDA "has allowed drugs for cancer and other diseases to stay on the market even when follow-up studies showed they didn't extend patients' lives" or the makers did not perform follow-up studies. The report criticizes the FDA's "so-called 'accelerated approval' program, which is only used to approve drugs for the most serious diseases." The program allows drugmakers to bring products to market sooner under the condition that they conduct follow-up studies. The GAO "identified several drugs still on the market that never lived up to their initial promise" and noted that in the program's 16 years the agency "never once pulled a drug off the market due to missing or unimpressive follow-up data." The Chicago Tribune (10/26) also covers the story. General Medical NewsH1N1 pandemic poses unique problems for heart, lung transplant patients, experts say.MedPage Today (10/23, Smith) reported, "The pandemic H1N1 flu poses special problems for people getting heart and lung transplants, according to an advisory from the International Society for Heart and Lung Transplantation." The authors, led by Lara Danziger-Isakov, MD, of the Cleveland Clinic Children's Hospital, fleshed out a number of "key elements" in lessening the pandemic's impact in the Journal of Heart and Lung Transplantation. Among the suggestions is the notion that "transplant patients should get both the seasonal trivalent inactivated flu vaccine and the H1N1 vaccine as soon as possible." In addition, "potential donors should have nasopharyngeal and throat swabs for the H1N1 virus before the organs are harvested." What's more, caregivers should "consider postexposure prophylaxis and prolonged seasonal prophylaxis, both with oseltamivir (Tamiflu)." Law and Policy
House, Senate Democratic leaders near agreement on some form of public option.Coverage of the healthcare debate focuses on what the Washington Post calls a "dramatic" shift in momentum back toward some form of public option plan being included in the final bill. NBC Nightly News (10/23, story 6, Williams) reported there are "signs that Congress may include" the public option. The House and Senate "are working to reconcile their different versions of the legislation. Both the Speaker of the House and the Senate Majority Leader are said to be supporting at least some version of it." Bloomberg News (10/24, Rowley, Litvan) similarly reports Senate Democrats "are leaning toward including a government-run insurance plan...that would let individual states to opt out, a proposal House leaders signaled would be acceptable." The Washington Post (10/24, A1, Murray, Montgomery) reported on its front page that Democratic leaders in both chambers "have concluded that a government-run insurance plan is the cheapest way to expand health coverage, and they sought Friday to rally support for the idea, prospects for which have gone in a few short weeks from bleak to bright." The Post called the "shift in momentum is so dramatic that many lawmakers now predict that President Obama will sign a final bill that includes some form of government-sponsored insurance for people who do not receive coverage through the workplace." The Los Angeles Times (10/24, Levey, Oliphant), the New York Times (10/24, A10, Pear, Herszenhorn), The Hill (10/23, Allen, Hooper), and the Washington Times (10/24, Haberkorn, Rowland) also covered the story. Some state, local lawmakers aiming to restrict e-cigarettes.USA Today (10/26, Koch) reports, "Electronic cigarettes are opening a new front in the tobacco wars as state and local lawmakers try to restrict the product." Although the industry maintains that "people who smoke ought to have better alternatives," a number of "public health officials question the safety of e-cigarettes." The FDA has even said that "the e-cigarettes it tested had carcinogens." But, while "distributors have filed a lawsuit challenging the FDA's authority," California attempted to pass "a ban on e-cigarette sales," only to be vetoed by Gov. Arnold Schwarzenegger (R). In addition, "Oregon Attorney General John Kroger, a Democrat, reached a settlement in August with retailers and distributors not to sell them," while lawmakers in New Hampshire and New Jersey work to ban their sale to minors and "subject e-cigarettes to the same restrictions as cigarettes," respectively. LATimes calls for regulation of e-cigarettes. The Los Angeles Times (10/26) editorializes, "E-cigarettes are the latest of a wave of nicotine-packing products...to face the wrath of the US Food and Drug Administration." Manufacturers maintain that the agency "has no jurisdiction over their merchandise because...it is not a smoking-cessation product." Yet, "in their zeal to avoid regulation...spokesmen for this fast-growing business have been engaging in doublespeak." On one hand, they claim the e-cigarette is "just a 'smoking alternative,' and in the same breath tout their superiority over gum or patches as a way to divert smokers from tobacco products." But, "with their candy flavors and their image as relatively harmless, e-cigarettes provide a new way to hook customers -- including teenagers -- on nicotine." So, "the public needs federal oversight of attempts to advance an addictive drug," while the product's safety is determined. Also in the NewsIT companies say software is crucial to providing more effective, efficient healthcare.The Chicago Tribune (10/26, Chan) notes that while the "rest of the world has embraced email, online forms and iPhone apps," healthcare still "communicates in the centuries-old technology of paper." For the last "four years," however, a "raft of tech companies" have been "making a major push into developing software for the healthcare industry." With Congressional leaders debating "how to provide coverage to the uninsured and the disparities in costs," IT companies are saying that "software is key to providing more effective and efficient care." For example, the Microsoft Health Solutions Group has developed "two products: HealthVault, a system to store electronic medical records, and Amalga, a database platform for large hospitals and pharmaceutical companies." Notably, the "federal economic stimulus package...includes funding for hospitals that switch to EMRs, which could help Microsoft sell its healthcare software." |
||||||
Subscriber Tools
Advertise with Custom Briefings:
Reach key professionals every morning
|
||||||
|
ATS Morning Minute is a digest of the most important news selected
from thousands of sources by the editors of Custom Briefings. The
American Thoracic Society does not select or edit the news items
contained herein, nor does it receive revenue from any advertising
herein. The views and opinions expressed herein do not necessarily
state or reflect those of the American Thoracic Society, and any
reference to specific commercial products, process, or service by
trade name or otherwise does not constitute or imply an endorsement
by the American Thoracic Society. Neither Custom Briefings nor the
American Thoracic Society is liable for the use of or reliance on
any information contained herein.
This complimentary copy of ATS Morning Minute was sent to jtavares5@aol.com as part of your ATS membership. View Custom Briefings' privacy policy. For more information about other ATS member benefits, please visit www.thoracic.org/sections/membership/benefits-of-an-ats-member.html or email membership@thoracic.org. American Thoracic Society | 61 Broadway | New York, NY 10006 Copyright © 2009 by Custom Briefings | 11190 Sunrise Valley Drive, Suite 130 | Reston, VA 20191 |
Pandemia ou pandemónio?
Manuel C. Mendonça *
26.10.2009
Começou
hoje a vacinação
contra a gripe A na Alemanha e possivelmente também noutros países pelo mundo
fora. Cerca de 80% da população da Alemanha não quer deixar-se vacinar contra
a gripe A, porque não tem nada de anormal.
A Suécia vacinou e de momento a tendência contra a segunda dose é abismal, face às reacções adversas da vacina. A imprensa internacional não fala doutra coisa.
Tecnicamente já se está a fugir da denominação gripe suína – um tanto ou quanto sem nexo - porque os suínos, esses sim, ainda continuam sem gripe.
O porquê da vacinação já foi sobejamente abordado pelas diversas fontes (independentes) de informação, porque, no que respeita aos doentes que contraíram o vírus, os sintomas em geral são muito leves.
Quem estará a tirar proveito deste pandemónio?
Porque duma pandemia, cuja definição sofreu uma recente alteração pela parte da OMS a proteger outros interesses, não se pode falar.
O que está bem claro neste drama actual, é a necessidade premente de algumas instituições em vacinar o maior número possível de indivíduos. Com que propósito?
Salvar vidas?
Eis alguns ingredientes da vacina:
Mercúrio, Formaldeído, Aspartame, Tiomersal, Fosfato de alumínio, Soro fetal bovino, Transplante de tecido fetal, Células renais do macaco, Glutamato de sódio, etc.
Esta mistela nada tem a ver com o propósito de salvar vidas. Que nos contem outras histórias, porque esta já nem um recém-nascido consegue embalar.
Não quero aprofundar este tema, mas para facilitar certas informações concretas, deixo aqui ficar alguns Links, cujos conteúdos ainda hão-de fazer arrepiar a pele a um ou outro que ainda acredita, que toda esta encenação tem o mero propósito de nos salvar duma pandemia.
http://www.theoneclickgroup.co.uk/news.php?start=2760&end=2780&view=yes&id=3581#newspost
Patente da vacina da gripe A foi registada pela firma Baxter 1 ano antes da epidemia!! Tudo bem orquestrado, como sempre!
http://www.theoneclickgroup.co.uk/documents/vaccines/Baxter%20Vaccine%20Patent%20Application.pdf
Patente da Baxter com requerimento datado de Agosto de 2008.
http://www.prisonplanet.com/flashback-another-flu-pandemic-causing-accident-occurred-in-2005.html
Quando se trata duma epidemia, está sempre um laboratório em jogo. Neste caso houve um “acidente propositado” com estirpes virulentas.
O maior perigo não é a gripe, mas sim a vacina. Muito interessante.
Gripe suína de 1976 e a catástrofe da vacinação em massa.
http://www.anovaordemmundial.com/2009/08/vacinacao-contra-gripe-suina-de-1976-60.html
http://www.anovaordemmundial.com/2009/09/epidemiologista-afirma-que-oms-alterou.html
http://www.apfn.org/apfn/aids.pdf
Documento do Ministério da Defesa dos EUA. Muito comprometedor acerca das origens do HIV e das entidades envolvidas neste pacto desumano. Leiam por favor e divulguem.
Por estas e mais outras razões não me deixo vacinar e nem aconselho a vacinar contra a gripe suína (gripe A). Alguns dos nossos irmãos na distante África, por falta de recursos, não vão ser vacinados. E estou convicto que vão sobreviver apesar do pandemónio. O importante em tudo isto é a higiene no nosso dia-a-dia.
Um grande abraço a todos e nada de pânico.
Vamos continuar a trabalhar.
NHOMBA
* Diplomado e Doutorado em medicina-veterinária; Formado em economia de marketing e vendas.
Ainda sobre o swine flu (H1N1) - gripe porcina
|
|
J.TAVARES, MD, FCCP, FAASM
21.10.2009
1 - O
debate e as controvérsias continuam.
Alguns jornalistas e personalidades políticas estão a incrementar o medo sobre a vacina com alegações de camuflagens, tentativas do governo de controlar as
Como médico, baseado na minha experiência nos últimos 24
meses, e na leitura de dados, aconselho todos os meus doentes a tomarem a
vacina!
Como marido, pai, familiar e amigo, também aconselho a todos a tomar a vacina, a não ser que tenham contra-indicação absoluta.
Um grande abraço!
|
||||||||
|
||||||||
Leading the News
Pregnant women most threatened by H1N1 flu.On the front of its "Science Times" section, the New York Times (10/20, D1, McNeil) reports, "The group most threatened by swine flu and most in need of the new vaccine, world health authorities agree, is that of pregnant women." The CDC said on October 1 that "100 pregnant women had been in intensive care with swine flu and 28 had died," which federal officials call "the best argument...for the drawn-out, expensive effort to make a swine flu vaccine." The article details the tribulations of Aubrey Opdyke, who was hospitalized for four months and lost her baby after getting the H1N1 flu while pregnant. NBC Nightly News (10/19, story 4, 2:35, Williams) reported, "For weeks now here, we have been covering the spread of swine flu, which the CDC now says is everywhere and still spreading." The segment focuses on Kelsey Young, who died of H1N1 flu one week after giving birth to her daughter. NBC (Bazell) added that he daughter, Ava, "is perfectly healthy, and her grandparents hope the story of the mother she will never meet will serve as a reminder of the severe dangers to pregnant woman from the new flu virus." H1N1 vaccinations begin across US. Local papers continued to cover H1N1 vaccination efforts in their areas. Most articles mentioned not only the vaccination clinics, but also contained comments that vaccine doses were scarce and not arriving in the numbers previously expected. The Miami Herald (10/20, Tasker, Sampson) reports, "School-age children will get most of the first shipment of vaccines in South Florida, and remaining doses will go to private physicians and federal and county health clinics for those who are most at risk." Vaccinations began Monday. "In Miami-Dade, students at schools served by 'health teams'...can get vaccinated at school clinics" while those "at the remaining schools...will have to get vaccinated by private physicians or at county clinics." In contrast, Broward plans to have vaccines "administered at six schools this week...with plans to spread to every school in the district over the next four or five weeks." The AP (10/20, La Corte) reports, "Production problems have slowed the arrival of swine flu vaccine shots in Washington state, but state officials said Monday pharmacies and doctor's offices will have enough to get all the primary groups started this week." Washington State Health Department Secretary Mary Selecky said that "by mid-November, there should be plenty of vaccine shots in Washington State for everyone who wants it, although the pace of delivery has been about 30 percent slower than expected." The Richmond Times-Dispatch (10/20, Prestidge, Bacque) and the San Jose Mercury News (10/20, Sulek) also have reports. Hospitals restricting visitors over H1N1 concerns. The AP (10/20) reports, "Hospitals around the country are turning away visiting children and tightening restrictions on adults, too, in hopes of limiting spread of swine flu," while others "are trying education instead of rules, posting signs that urge people of any age to postpone that visit if they have a sniffle or cough." This is "a confusing time as hospitals struggle to balance the recuperative effects of having loved ones visit with the fear that they'll carry in swine flu to people already weakened from something else." Because the policies are made mostly on a hospital-by-hospital basis, this is leading to "huge variation," even in the same town. Meanwhile, "there's been little study of whether curbing visitors, or screening them for symptoms, keeps flu from sneaking into other parts of the hospital." Some churches alter routines to discourage H1N1 transmission. The Wall Street Journal (10/20, Fields, Evans) reports on how some churches are altering their routines to minimize the transmission of H1N1 flu. This includes putting out hand sanitizer, limited hand-to-hand contact, and using individually wrapped bread and juice packets to share bread and wine during the mass. FDA considering emergency use authorization for Peramivir. The CBS Evening News (10/19, story 7, 3:15, Couric) reported, "More doses of H1N1 are due out this week, but what about people who already have the flu and are very sick? Some doctors say they would use a new experimental drug" -- Peramivir -- "to treat them if only they were allowed." Already, the FDA "has approved 20...requests for" the drug "under the law allowing the compassionate use of unapproved drugs." But "doctors want the FDA to speed up the delivery." At present, the "process now for compassionate use takes at least four hours of paperwork from doctors trying to treat sick patients. The FDA has said it will consider what's called an EUA, emergency use authorization, for Peramivir, allowing the government to stockpile the drug and reduce the paperwork." The CBS website has a text version of this story. NIH study to determine dose of H1N1 vaccine for those with asthma. WKYC-TV Cleveland (10/19) reported on its website, "The National Institutes of Health is preparing to launch the first government-sponsored clinical trial to determine what dose of the 2009 H1N1 influenza vaccine is needed to induce a protective immune response in people with asthma." The study, cosponsored by the National Institute of Allergy and Infectious Diseases and the National Heart, Lung, and Blood Institute, "will determine the optimal dose of 2009 H1N1 influenza vaccine that can be safely administered to this at-risk population and whether one or two doses are needed to produce an immune response that is predictive of protection." Its "plan has been submitted to the Food and Drug Administration for review." California nurses threaten strike over H1N1 protections. The AP (10/19, Mohajer) reports that the California Nurses Association has threatened a one-day strike at 34 hospitals, accusing the providers of poor swine flu preparedness" and seeking state and federal swine flu protection recommendations to be written into their contracts. CQ HealthBeat (10/19) reports, "The nurses say hospitals are not doing enough to isolate patients with H1N1 symptoms and are not providing enough fit-tested N95 respirators and other protective gear." They "also say that hospitals are not adhering to safe staffing ratios required by state law and that nurses are being harassed by supervisors to accept unsafe assignments and not take breaks." The California Nurses Association and the National Nurses Organizing Committee says that "as many as 16,000 nurses in California and Nevada could join the protests." The Wall Street Journal (10/20, Maher) also covers this story. Author says H1N1 is "a pandemic in name only." In an op-ed in the Washington Times (10/20), author Michael Fumento, director of the Independent Journalism Project, writes that H1N1 flu is "a pandemic in name only." In "a so-called 'plausible scenario' in a report from the President's Council of Advisors on Science and Technology" 30,000 to 90,000 deaths were predicted, peaking around now, because the Council "assumed swine flu would behave as a pandemic." However, Fumento asserts that "data from all over the world showed that swine flu is far milder than the seasonal variety," with the Southern Hemisphere seeing "fewer flu deaths than normal." He recommends people consider getting vaccinated but concludes, "Just because somebody issues a proclamation, don't believe that Piglet has become a raging razorback." ResearchStudy suggests acetaminophen makes vaccines less potent.The New York Times (10/20, D6, McNeil) reports that a new study financed by GlaxoSmithKline, "done in the Czech Republic and published last week in The Lancet," found that acetaminophen "makes some vaccines less potent." The authors wrote that "fever is part of the immune response, and suppressing it...appeared to impair the body's ability to make antibodies." While "the authors said their findings needed 'further assessment'," they "suggested that antifever medication not be given routinely but only when needed." CDC researchers said in an editorial that the "study offered 'a compelling case' against routine dosing but that the issue required more study. Pulmonary embolism, deep vein thrombosis may not always co-exist in trauma patients, research suggests.Medscape (10/19, Barclay) reported, "Few trauma patients with pulmonary embolism (PE) have pelvic or leg deep venous thrombosis (DVT), suggesting that PE may occur de novo in the lungs," according to a paper in the Archives of Surgery. Harvard researchers, alongside investigators at Massachusetts General Hospital, explained that "for decades, it has been taught that [PE] is a sequel of [DVT]" because "forming in the lower extremity or pelvic veins, clots break off and travel to the pulmonary circulation." Thus, DVT and PE "should coexist in most patients, because part of the clot embolizes in the lung, and part remains attached to the vein." But, MedPage Today (10/19, Smith) reported, after conducting a "single-center retrospective analysis of nearly 250 patients" who were evaluated using "computed tomographic venography" and angiography, investigators noted that, "over the three-year period...46 patients had a pulmonary embolism and 18 had a deep vein thrombosis." But "only seven patients with a pulmonary embolism also had a deep vein clot -- or 15 percent of the 46." Although there may be several reasons for this, "the most likely explanation is that in trauma patients pulmonary emboli arise in the lungs in the first place and are not related to clots in the veins of the lower extremities."
Three-day antibiotic course may be sufficient for pediatric tonsillectomy patients, researchers say.MedPage Today (10/19, Smith) reported, "Three days of antibiotics after a tonsillectomy will put kids back on a normal diet and activity level," according to a paper in Archives of Otolaryngology-Head & Neck Surgery. "Several studies have demonstrated that postoperative antibiotics reduce pain, thought to be caused when normal oral bacteria colonize the tonsillar fossae and cause inflammation." And "for that reason, most otolaryngologists prescribe antibiotics after the procedure -- usually for seven days." But, after evaluating 49 pediatric patients, researchers at New York Presbyterian Hospital-Weill Cornell Medical College found that "there was no difference between three and seven days of antibiotics in the time it took to get back to normal." Regulatory newsFDA approves Glaxo seasonal flu vaccine for children.The AP (10/20) reports, "GlaxoSmithKline PLC said Monday the Food and Drug Administration approved the seasonal flu vaccine Fluarix for children." While previously approved for adults, it is now approved for children ages three to 17 years old. FDA requests more information on Novartis' COPD drug.The Wall Street Journal (10/20, Greil) reports that the FDA on Monday requested more information on the dosing proposed for Novartis AG's indacaterol, or QAB149, which is an experimental treatment for chronic obstructive pulmonary disease. Novartis said it will work with the FDA to review already-submitted data and recent data to decide which, if any, clinical trials will be needed. Last month, European regulators recommended the drug for approval. General Medical News
Investigators say timing matters greatly in administering supplemental oxygen to reduce brain damage in stroke patients.HealthDay (10/19, Dotinga) reported, "Contradicting previous research, scientists have shown in animal studies that providing supplemental oxygen during an ischemic stroke can reduce brain damage." But Ohio State University researchers are quick to point out that the success rate "depends on when 100 percent oxygen is given." Using "supplemental oxygen after blood flow is restored in the brain appears to actually cause harm by unleashing free radicals," and the "resulting tissue damage was worse than stroke-affected tissue that received no treatment at all." On the other hand, "supplemental oxygen during the blockage...is highly protective," the authors observed during their rodent experiment. Law and PolicySen. Reid backing bill to halt Medicare physician reimbursement cuts.The Los Angeles Times (10/20, Geiger) reports that Senate Majority Leader Harry Reid (D-NV) is backing a bill introduced by Michigan Sen. Debbie Stabenow (D) to "reconcile a nearly $250-billion difference between the House and Senate approaches to overhauling healthcare" by halting "scheduled reductions in Medicare payments to physicians." Sen. Stabenow's bill "would end the cuts and set Medicare payment rates at current levels. Doing so would allow Democrats to maintain the American Medical Assn.'s support for an overhaul without having to absorb the cost of higher doctor payments in the final healthcare bill." The Times explains that Congress has deferred cuts at the AMA's behest for a number of years, resulting in a 21% cut scheduled for next year. The AP (10/20, Espo) notes that despite the movement, the "AMA won't yet pledge support for the major healthcare bill" despite numerous requests, and it also does not seem "eager to soft-pedal another of its own top priorities, legislation to restrict medical malpractice payments." CongressDaily (10/20), meanwhile, reports that Ohio Sen. Sherrod Brown (D) announced Monday afternoon that there could be a cloture vote on the bill "as early as [Tuesday] afternoon if both parties' leaders agree. Health reform bills allow age disparity in insurance premiums.McClatchy (10/20, Lightman) reports that though current legislation in the House and Senate would allow health insurers to continue charging older beneficiaries more than their younger counterparts, they "would end what many consider another longstanding, discriminatory practice -- basing rates on gender, which is now allowed in most states. Some wonder, are middle-aged and older consumers victims of age discrimination? Senate Finance Committee member John Kerry (D-MA) said, 'Allowing insurers to charge older Americans vastly higher premiums simply because of their age is discrimination, pure and simple.'" However, "Lawmakers explained that charging older people more, though, also could be justified with data." Practice Management
"Medical home" model profiled.The Chicago Tribune (10/20, Graham) profiles the "medical home" model emerging in parts of the country, which the Tribune describes as "primary care on steroids, devoted to prevention and to helping people with chronic conditions such as asthma or arthritis manage their illness." Under the model, physicians oversee teams of health professionals charged with closely monitoring patients' health. Illinois' largest health insurer has explored the model with a pilot program, and Medicare "announced a similar initiative" last month. In order to succeed, "the way doctors are paid has to change fundamentally," according to the chief executive of the Mercy Clinics, Inc. Dr. David Swieskowski also pointed out that doctors may be resistant to a structure in which they are ultimately "accountable for results, such as how many diabetic patients have blood sugar adequately controlled." Also in the NewsThree drugmakers settle Medicaid claims with US.The AP (10/20) reports that Mylan, Inc. "will pay $121 million to settle claims it did not properly reimburse Medicaid for drugs, while two other drugmakers are making smaller payments." The AP adds, "Two Mylan subsidiaries, along with units of AstraZeneca PLC and Johnson & Johnson, are resolving allegations they sold drugs to Medicaid and then reimbursed the program at a lower rate. The settlements resolve allegations the companies violated the False Claims Act between 2000 and 2004." Mylan "says it will take a one-time charge of $83 million in the third quarter, but will try to recover some of the funds from third parties that supplied it with products and received overpayments." |
||||||||
Subscriber Tools
Advertise with Custom Briefings:
Reach key professionals every morning
|
||||||||
|
ATS Morning Minute is a digest of the most important news selected
from thousands of sources by the editors of Custom Briefings. The
American Thoracic Society does not select or edit the news items
contained herein, nor does it receive revenue from any advertising
herein. The views and opinions expressed herein do not necessarily
state or reflect those of the American Thoracic Society, and any
reference to specific commercial products, process, or service by
trade name or otherwise does not constitute or imply an endorsement
by the American Thoracic Society. Neither Custom Briefings nor the
American Thoracic Society is liable for the use of or reliance on
any information contained herein.
This complimentary copy of ATS Morning Minute was sent to jtavares5@aol.com as part of your ATS membership. View Custom Briefings' privacy policy. For more information about other ATS member benefits, please visit www.thoracic.org/sections/membership/benefits-of-an-ats-member.html or email membership@thoracic.org. American Thoracic Society | 61 Broadway | New York, NY 10006 Copyright © 2009 by Custom Briefings | 11190 Sunrise Valley Drive, Suite 130 | Reston, VA 20191 |
|
||||||||
|
||||||||
Leading the News
H1N1 flu vaccine concerns said to be aiding anti-vaccine movement.In a front-page article, the New York Times (10/16, A1, Steinhauer) reports that health experts say that "an assemblage of factors around the swine flu vaccine -- including confusion over how it was made, widespread speculation about whether it might be more dangerous than the virus itself, and complaints among some healthcare workers in New York about a requirement that they be vaccinated -- is giving the anti-vaccine movement a fresh airing." The issue "is frustrating to health officials, who are struggling to persuade an already wary public to line up for shots and prevent the spread of the pandemic." Health officials are also "concerned that some groups, especially pregnant women, are potentially swayed by the large-scale efforts of vaccine opponents." Talk-show hosts seen as stoking anxiety about H1N1 vaccine. The Washington Times (10/16, Bunch) reports, "Over the past few weeks, several prominent talk-show hosts from across the political spectrum," including Bill Maher, Rush Limbaugh, and Glenn Beck, "have stoked public anxiety about the swine flu vaccine." Tom Skinner, the senior public affairs officer at the CDC, said it is "worrisome...that those who are critical of vaccination often do not base their opinions on sound scientific information." Meanwhile, Tevi Troy, deputy secretary of health and human services in the Bush Administration, said that although "you can't trust the government for the administration of healthcare...that doesn't mean that there aren't very good scientists at the CDC, at the [Food and Drug Administration], at the [National Institutes of Health] who help us develop cures and who help us plan our public healthcare responses to bioevents." Hospitals may not be able to handle surge of H1N1 patients. NBC Nightly News (10/15, story 10, 2:20, Gregory) reported, "Recent studies have shown the key role of hospital intensive care units and especially a complex device that is a combination of a heart/lung machine and respirator in saving lives of those who have these severe complications associated with the flu. But are hospitals prepared if the epidemic gets worse?" NBC (Bazell) added, "Because the ECMO machines are so successful at treating so many very bad conditions in hospitals that have them, they're in almost constant use already." Bazell noted, "In most hospitals, everything in the ICU is at 95% capacity." Dr. Douglas White of the University of Pittsburgh was shown saying, "Most hospitals don't have robust plans on how to increase the capacity of their hospital to deal with a big surge of patients requiring intensive care." FDA urges consumers to avoid buying H1N1 treatments online. CNN (10/16) reports that the FDA is warning Americans to "avoid buying treatments for the H1N1 virus, commonly known as swine flu, online." FDA Commissioner Margaret Hamburg said, "Products that are offered for sale online with claims to diagnose, prevent, mitigate, treat or cure the 2009 H1N1 influenza virus must be carefully evaluated." She added, "Medicines purchased from websites operating outside the law put consumers at increased risk due to a higher potential that the products will be counterfeit, impure, contaminated or have too little or too much of the active ingredient." The Los Angeles Times (10/15, Maugh II) "Booster Shots" blog and Dow Jones Newswire (10/16, Favole) also cover the story. New York medical workers sue to stop H1N1 vaccinations. AFP (10/15) reported that New York medical workers "filed a temporary restraining order in a Washington federal court against government medical regulators they claim rushed H1N1 vaccines to the public without adequately testing their safety and efficacy." Jim Turner, one of half a dozen lawyers working on the case, "insisted that 'the FDA did not do the proper testing to show safety and efficacy of this vaccine, which is under the law a new drug.'" The plaintiff also "argued that far from preventing a massive outbreak of swine flu, the 'live attenuated influenza virus nasal mist vaccine could trigger' an H1N1 pandemic." However, "officials at the National Institutes of Health have said that trials of swine flu vaccine" found it "was well tolerated and produced a robust immune response in older children and adults in good health with just a single dose." Seasonal flu vaccine in short supply. The San Antonio Business Journal (10/15) reported, "A national shortage of seasonal flu vaccines is prompting WellCheck Medical Centers to cancel its planned clinics at Simon Property Group shopping centers." Jack Tawil, CEO of WellCheck Medical Centers, said that "the vaccination shortage is...a national issue." The Bangor (ME) Daily News (10/16, Haskell) reports, "Vulnerable nursing home residents and schoolchildren are among the Mainers being told they will have to wait for a vaccination against seasonal influenza," because "Fewer than half of the approximately 300,000 doses of seasonal flu vaccine ordered by the Maine Center for Disease Control and Prevention have been delivered to date." Agency director Dr. Dora Anne Mills "says it probably will be late November before all the ordered vaccine is distributed." She "said the delay is being caused by a bottleneck in the vaccine manufacturing process due to the competing demand for H1N1 swine flu vaccine." ResearchResearch confirms smoking bans reduce heart attacks in nonsmokers.ABC World News (10/15, story 9, 0:20, Gibson) reported that research commissioned by the Centers for Disease Control and Prevention "finds smoking bans are effective when it comes to cutting the risks to nonsmokers." The New York Times (10/16, Belluck) reports that "smoking bans in places like restaurants, offices and public buildings reduce cases of heart attacks and heart disease, according to" the report. A panel of scientists "extensively examined the published and unpublished data on the connection between secondhand smoke and heart problems, focusing particularly on 11 studies from different communities in Canada, Italy, Scotland and the United States that had imposed bans on smoking." The Wall Street Journal (10/16, Becker, Cordeiro) reports that the scientific panel said, "The repeated finding of decreased heart attack rates overall after bans were implemented conclusively demonstrates that smoke-free policies help protect people from the cardiovascular effects of tobacco smoke." The AP (10/16, Neergaard) reports that "while heavier exposure to secondhand smoke is worse, there's no safe level," according to the report. The report "also cited 'compelling' if circumstantial evidence that even less than an hour's exposure might be enough to push someone already at risk of a heart attack over the edge." The Los Angeles Times (10/16, Maugh II), Reuters (10/16, Morgan), WebMD (10/15, Boyles), HealthDay (10/15, Reinberg), the UK's Daily Mail (10/16), and AFP (10/16) also cover the story. Research suggests diet, exercise alone fails to cure OSA in obese patients.Medscape (10/15, Barclay) reported, "Diet and exercise alone may fail to cure obstructive sleep apnea (OSA) in obese patients," researchers in Australia found after enrolling 12 people in a 16-week program. "Following a proprietary, very low energy diet (Optifast, Novartis) and an exercise schedule of aerobic and resistance training supervised by a physiologist and a physiotherapist," investigators noted that "weight loss was significant among 10 participants who completed the program." But while "there was some improvement in sleep disordered breathing, it was not seen in all patients and was not proportional to the degree of weight loss," the authors concluded in Journal of Clinical Sleep Medicine. Analysis indicates pleiotropic effects of statins may help against some infections.HeartWire (10/15, O'Riordan) reported that "the pleiotropic effects of statins are useful in the treatment and prevention of different infections, including bacteremia, pneumonia, and sepsis," according to an analysis published in the Archives of Internal Medicine. Researchers found that "in nine studies that looked at the treatment of infections with statins, the pooled adjusted effect favored the use of the drugs, including effects on end points such as 30-day mortality and 30-mortality due to infection." Meanwhile, "in seven prevention studies, including those in the setting of chronic kidney disease, vascular disease, and the intensive-care unit, treatment with statins reduced the risk of developing an infection." Regulatory newsFDA says warning to P&G over Vicks was posted in error.The Cincinnati Enquirer (10/15) reported that the FDA "says it never issued a warning letter to Procter & gamble over P&G's Vicks product." While "a warning letter appeared on the FDA's website Wednesday warning P&G against adding vitamin C to some of its Vicks formulas," the agency "said the letter was posted online due to an internal error and that no warning was actually issued to the company." FDA spokesman Chris Kelly said in a statement, "The agency regrets any confusion caused by the posting." MedPage Today (10/15, Gever) pointed out that "the statement did not indicate whether the agency still had concerns about the inclusion of vitamin C in the products or their labeling." The Chicago Tribune (10/16), the AP (10/16), Dow Jones Newswires (10/16, Dooren), and Reuters (10/16, Richwine, Klayman) also covered this story.
FDA issues new guidelines on drug disposal.MedPage Today (10/15, Petrochko) reported, "The FDA has issued new consumer guidelines for disposing of unused or expired medications that might be dangerous to others." The list of drugs "includes high-potency opioids and other controlled substances that may be harmful or deadly in as little as single doses if taken by someone other than the prescribed patient." Drugs to be disposed of by flushing down a sink or toilet include "a number of fentanyl, morphine, and oxycodone-based drugs." But, the FDA "said most medications are not recommended for flushing and should instead be mixed with an unpalatable substance, such as coffee grounds or kitty litter, placed in a sealed plastic bag, and thrown in the trash." General Medical News
Using acetaminophen following vaccination may reduce efficacy, research suggests.The Los Angeles Times (10/15, Maugh II) "Booster Shots" blog reported, "Giving acetaminophen -- best known by the brand-name Tylenol -- to infants along with vaccines to prevent fevers from developing reduces the effectiveness of the vaccines." A number of parents swear by the acetaminophen regimen, "and some doctors recommend" it, the AP (10/16, Marchione) points out. The "CDC's vaccine advisory panel says it is a reasonable thing to do for children at high risk of seizures, which can be triggered by fevers." However, "military and government scientists in the Czech Republic" uncovered evidence that may undermine the practice after evaluating children at 10 medical centers. The "children were vaccinated against diphtheria, tetanus, poliomyelitis, hepatitis B, whooping cough, diarrhea-causing rotaviruses and Haemophilus influenzae type B," Bloomberg News (10/16, Fourcade) reported. Investigators then divided the 459 participants. "One group received three doses of" acetaminophen "after vaccination and the other didn't." Investigators noted "fewer infants who received acetaminophen had a fever, but these babies also had significantly fewer antibodies against pneumococcal disease, Haemophilus influenzae type b, diphtheria and tetanus toxoids, and for one of the whooping cough antibodies compared with infants who did not get acetaminophen," HealthDay (10/15, Reinberg) reported. After "booster doses at 12 to 15 months, children who received prophylactic acetaminophen still had reduced immune responses to the vaccines against pneumococcal disease, Hib, and tetanus," MedPage Today (10/15, Neale) reported. WebMD (10/15, DeNoon) and BBC News (10/16) also cover the story. Law and PolicySenate holds hearing on higher health insurance costs for women.ABC World News (10/15, story 7, 2:30, Gibson) reported, "On Capitol Hill today, lawmakers heard from women who battled their insurance companies, and say they have been forced to pay higher premiums for less coverage. In some cases, the women say their insurers tried to coerce them not to have children." ABC (Stark) added, "Lawmakers today were told that women are often charged more for health insurance, as much as 48% more than a man of the same age. Only 11 states forbid health insurance companies from basing premiums on gender." Stark continued, "All the health reform bills being debated right now tackle this problem, forbidding insurance companies from considering gender or pre-existing conditions." CQ HealthBeat (10/15, Norman) reports that Karen Ignagni, president and chief executive of America's Health Insurance Plans, told the Senate Health, Education, Labor, and Pensions committee that "the nation's health insurers are fully committed to ending policies that charge women higher premiums or deny them coverage because of their age, gender or 'pre-existing conditions' such as pregnancy," but she "also said repeatedly that healthcare overhaul legislation approved by Congress must ensure an individual mandate is included in which every American is required to obtain health coverage." McClatchy (10/15, Bolstad) reports, "At Thursday's hearing, many women had examples of individual policies that require women to pay more than men." James Guest, the president and chief executive of Consumers Union, testified that "Women already face a number of hurdles when it comes to healthcare," saying, "For women, the health insurance crisis is very real, very personal, and very scary." Medicaid to cover smoking-cessation drugs under reform legislation.The Wall Street Journal (10/16, Mundy) reports that while healthcare legislation has made its way through the Senate Finance Committee, it contains smaller-item provisions that may fuel debate among certain groups. For instance, Medicaid patients could gain increased access to medicines like Chantix (varenicline) and Zyban (bupropion). The American Cancer Society says it would like to eventually see a greater variety of cancer-preventing drugs and therapies covered by Medicare and Medicaid, as well as private insurance. Practice Management
Research indicates being mindful may improve physicians' well-being, sharpen clinical skills.In the New York Times (10/15) Doctor and Patient column, Pauline W. Chen, MD, wrote, "Extreme multitasking has" not only "invaded the patient-doctor relationship," but it has also "contributed to high rates of burnout among physicians." However, according to a recent study published in the Journal of the American Medical Association, many physicians who participated in "a year-long course...on mindfulness" felt "less burned out and less emotionally exhausted." The study also showed that "several of the improvements persisted even after the yearlong course ended," which "correlated with a significant increase in attributes that contribute to patient-centered care." Dr. Michael S. Krasner, lead author of the study and an associate professor of clinical medicine at the University of Rochester, noted that "acquiring the ability to be mindful in the most challenging circumstances can do more than improve a physician's well-being; it can also sharpen clinical skills." Also in the NewsAppeals court says specific diagnostic test patentable.American Medical News (10/15, Sorrel) reported that a federal appeals court "ruled that a diagnostic test for determining proper drug dosages to treat certain diseases is patentable under federal law." Prometheus Laboratories, Inc. alleged that Mayo Collaborative Services infringed "on its patents" on a test to measure "metabolite levels in patients taking thiopurine drugs" and correlate "those levels with the drug's efficacy." For its part, Mayo argued that "Prometheus' patents were invalid because they covered naturally occurring phenomena." The appeals court, however, sided with Prometheus, ruling that "the patent was permissible because it involved a new application of a fundamental principle." Meanwhile, "according to a friend-of-the-court brief filed in support of Mayo by" several "medical organizations," physicians are now "concerned that allowing such broad patents will give companies a monopoly over...medical research that should be shared." |
||||||||
Subscriber Tools
Advertise with Custom Briefings:
Reach key professionals every morning
|
||||||||
|
ATS Morning Minute is a digest of the most important news selected
from thousands of sources by the editors of Custom Briefings. The
American Thoracic Society does not select or edit the news items
contained herein, nor does it receive revenue from any advertising
herein. The views and opinions expressed herein do not necessarily
state or reflect those of the American Thoracic Society, and any
reference to specific commercial products, process, or service by
trade name or otherwise does not constitute or imply an endorsement
by the American Thoracic Society. Neither Custom Briefings nor the
American Thoracic Society is liable for the use of or reliance on
any information contained herein.
This complimentary copy of ATS Morning Minute was sent to jtavares5@aol.com as part of your ATS membership. View Custom Briefings' privacy policy. For more information about other ATS member benefits, please visit www.thoracic.org/sections/membership/benefits-of-an-ats-member.html or email membership@thoracic.org. American Thoracic Society | 61 Broadway | New York, NY 10006 Copyright © 2009 by Custom Briefings | 11190 Sunrise Valley Drive, Suite 130 | Reston, VA 20191 |
Ainda sobre o swine flu (H1N1) - gripe porcina
|
|
J.TAVARES, MD, FCCP, FAASM
07.10.2009
Chegou hoje à minha caixa de correio, através do Didinho, um excerto de algumas declarações do Bastonário da Ordem dos Médicos Portugueses. Não podia perder
esta oportunidade para comentar.
Em tempo de crise, o papel de um líder é de acalmar as pessoas, evitar que entrem em pânico. Até aqui, tudo bem, o Dr. Pedro Nunes cumpriu o seu papel; mas dizer
que o H1N1 é uma “doença banal, pouco letal, banalíssima” é no mínimo irresponsável. Diga isso ao Dr. Guillermo Dominguez-Cherit (Mexico City) que foi dos
primeiros intensivistas a tratar de doentes nos cuidados intensivos que contraíram o H1N1 (dos doentes entre os 20 e os 55 anos e que necessitaram de ventilador,
75% deles morreram). Em geral, durante esse período, das 3646 pessoas que contraíram o H1N1, 70 (quase 2%) morreram. Diga isso à senhora de 41 anos, com 3
filhos, cujo marido que era saudável até há 6 meses atrás, contraíu o H1N1 tendo falecido, apesar de todos os nossos esforços (tive que estar envolvido no caso que era
num hospital a que geralmente não vou, porque necessitavam de um “expert” em Osciladores de Alta Frequência); Diga isso à senhora originária da Polinésia
(caso que relatei no CONTRIBUTO meses atrás) e a um jovem de 35 anos que 2 meses atrás esteve as portas da morte por 2 semanas - felizmente estes 2 casos
sobreviveram...
Acalmar as "tropas", sim, mas não desleixar, não deixar que as "tropas" baixem a guarda, porque pode ser catastrófico!
Imagine-se um trabalhador da Saúde com o Vírus, transmiti-lo a doentes nos Hospitais!!!
Há sempre cepticismo, por todo o lado: mais uma propaganda para vender vacinas, máscaras, luvas, etc.; em tudo, há sempre um pouco de verdade, mas este vírus “is real”; todos temos de tomar as precauções necessárias para prevenir a sua transmissão. Nada de pânico, mas também, nada de displicência.
Regularmente, vou compartilhar com os leitores do CONTRIBUTO, vários “customized briefings” enviados para mim pela American Thoracic Society e que podem ler e tentar formar uma opinião.
Por falta de tempo, não vou poder traduzir (de vez em quando, vamos publicando comentários sobre os “briefings”.
Obrigado!

Beja, 06 Out (Lusa) -- O bastonário da Ordem dos Médicos criticou hoje o "excesso de alarme e zelo" na resposta à gripe A H1N1, considerando tratar-se de uma "doença banal e pouco letal"."Há claramente um excesso de alarme, de zelo", disse Pedro Nunes, referindo que "não passa de uma gripe, uma doença banal, pouco letal". Neste sentido, frisou, "o melhor contributo da Ordem dos Médicos é chamar a atenção dos médicos e, através deles, das pessoas, de que isto é uma doença banalíssima e que não é preciso andarmos todos assustados". |
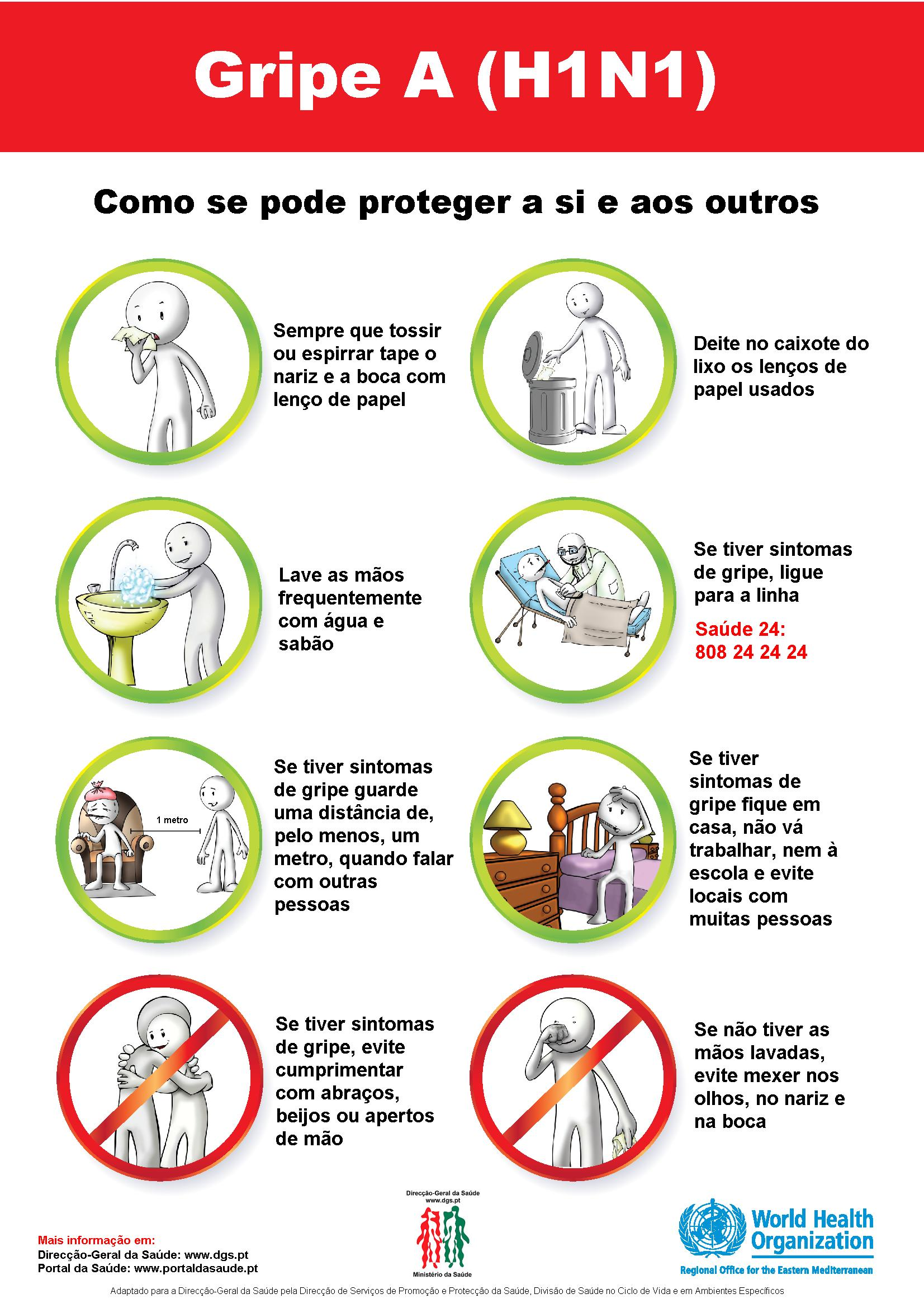
![]()
![]() ESPAÇO
PARA COMENTÁRIOS SOBRE A SAÚDE -- PARTICIPE!
ESPAÇO
PARA COMENTÁRIOS SOBRE A SAÚDE -- PARTICIPE!
![]()
VAMOS CONTINUAR A TRABALHAR!
Projecto Guiné-Bissau: CONTRIBUTO